Introduction
Sarcoidosis is a complex, multi-organ inflammatory disease which can have various systemic and ocular manifestations. The lungs, lymph nodes, skin, eyes, liver, heart, and central nervous system (CNS) are among the organs affected. In the eye, sarcoid can affect many structures including the eyelid, conjunctiva, anterior chamber, retina, and optic nerve. Ocular involvement is the presenting symptom in approximately 20-30% of cases of sarcoidosis.2 There is a rare subset of patients that present with only ocular sarcoidosis and the diagnosis is challenging due to the classic signs of sarcoid uveitis, such as those outlined by the first International Workshop on Ocular Sarcoidosis (IWOS) in 2009, are absent. This paper will outline a case of initially presumed ocular sarcoidosis which presented without the classic signs of sarcoid-associated uveitis to illustrate the complexity of the disease. The focus will be on ocular sarcoidosis with an emphasis on sarcoid related uveitis, diagnosis, and treatment/management. A multidisciplinary approach to the management of such a multi-organ condition will be highlighted.
Case Report
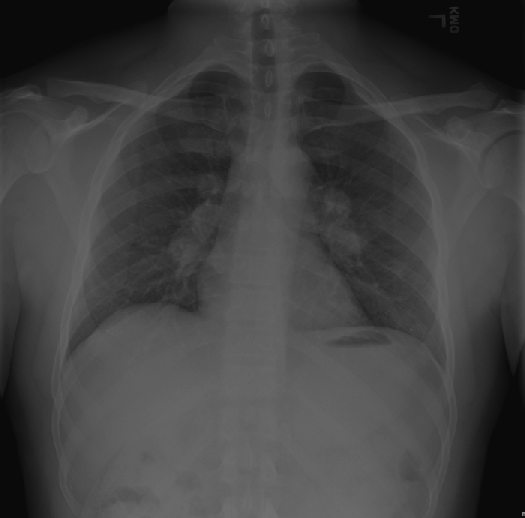
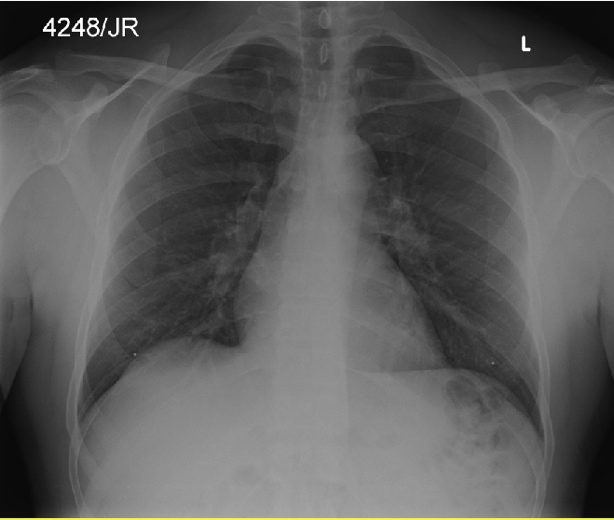
A 38-year-old African American male presented with a chief complaint of blurry vision and a pressure sensation behind his left eye. He reported that these symptoms started a few days prior and were worsening. Medical history was significant for presumed pulmonary sarcoidosis based on Chest X-ray results and lumbago. He was not taking any systemic medications aside from ibuprofen 800 mg as needed for pain relief. Ocular history was positive for mobile eyelid lesions on the upper orbital rim of both eyes noted three years prior. At that visit, blood work was normal except for a mildly elevated angiotensin converting enzyme (ACE) value. A chest X-ray was also obtained which revealed bilateral hilar adenopathy. Based on these findings, a diagnosis of presumed pulmonary sarcoidosis was made with no further biopsies ordered.
At the current visit, entering habitual visual acuity (VA) was 20/25-3 OD and 20/50+1 OS. After refraction, best corrected VA was 20/20 in each eye, with a 1.50 Diopter myopic shift OS. Pupils, extraocular motilities, and confrontational visual fields were unremarkable. The anterior segment examination revealed Grade 2+ cells and flare OD and Grade 3+ cells and flare OS and intraocular pressure (IOP) measured by Goldman applanation tonometry was 20 mmHg OD and 48 mmHg OS. Gonioscopy was performed secondary to elevated IOP and revealed open angles with no evidence of angle recession, peripheral anterior synechiae (PAS), or trabecular meshwork nodules OU. A dilated fundus examination was normal with a clear vitreous and no evidence of macular edema. The optic nerve heads showed small cupping with pink and distinct rim tissue and the peripheral retina was unremarkable in both eyes.
Based on the previous history of bilateral eyelid lesions, bilateral hilar adenopathy on chest X-ray, and now the presence of bilateral uveitis, ocular sarcoidosis was presumed. At this time, no further imaging or bloodwork was ordered. The patient was diagnosed with bilateral anterior non-granulomatous uveitis likely related to sarcoidosis and was started on prednisolone acetate ophthalmic suspension 1% QID OU. Due to the increase in IOP, he was also prescribed dorzolamide/timolol BID OU and brimonidine tartrate 0.2% BID OU.
Additional Examinations
At the one-day follow-up, the patient noted an improvement in vision and comfort of the eyes. Entering VA with correction was 20/20-3 OD and 20/20-1 OS. There was now Grade 1+ cells OD and 2+ cells OS and IOP measured 14mmHg OD and 17 mmHg OS. The treatment plan of prednisolone acetate 1% QID OU, brimonidine tartrate 0.2% BID OU, and dorzolamide/timolol BID OU was continued.
Over a one-month period, the anterior chamber reaction persisted at Grade 1+ cells OD and OS on prednisolone acetate 1% QID OU and IOP was maintained between 9-14 mmHg on brimonidine tartrate 0.2% BID OU and dorzolamide/timolol BID OU. Due to the prolonged inflammation, a repeat lab investigation was ordered to rule out other infectious and inflammatory causes of the anterior uveitis. A consultation was made with a uveitis specialist, and it was determined that the bilateral anterior uveitis was likely secondary to sarcoidosis and that it was safe to begin to taper the steroid and discontinue dorzolamide/timolol BID OU. The patient’s taper schedule was set for prednisolone acetate 1% TID OU x 2 weeks, BID OU x 2 weeks, and QD OU x 2 weeks.
During the above taper, the patient experienced an episode of rebound uveitis and increased IOP. Prednisolone acetate 1% was restarted and later switched to difluprednate ophthalmic emulsion 0.05% QID OU with a longer taper to prevent rebound effect. IOP was also controlled with brimonidine tartrate 0.2% BID OU.
The patient was examined biweekly until the anterior chamber was clear in each eye, IOP was normotensive in each eye without treatment, and the patient was asymptomatic. Based on his ocular manifestations and presumed ocular sarcoidosis diagnosis, the primary care provider was alerted for systemic follow-up. The patient was also evaluated by cardiology to monitor for any cardiologic manifestations, of which there were none.
Over the span of two years, the patient had two recurrences of anterior uveitis. Each time, he presented with complaints of ocular pain, mild photophobia, and tearing bilaterally. Exam findings were similar each time with best corrected visual acuity of 20/20 in both eyes. Anterior segment exam was notable for Grade 1+ cells - Grade 2+ cells with no flare in each eye at presentation and his IOP was elevated. Dilated fundus examination was normal with no posterior segment findings in both eyes. The patient was diagnosed with recurrent bilateral non-granulomatous anterior uveitis related to pulmonary sarcoidosis based upon prior medical history. Treatment was initiated with prednisolone acetate 1% hourly (q1h) OU, cyclopentolate 1% BID OU, and dorzolamide/timolol BID to lower IOP. A slow taper of prednisolone acetate was required over the course of 3 months on average before his iritis was resolved.
Two and a half years after the initial episode of uveitis, the patient developed constitutional symptoms of erectile dysfunction and nocturia. His bloodwork showed low total testosterone and luteinizing hormone and was diagnosed with hypogonadotropic hypogonadism. A pituitary process was suggested, and magnetic resonance imaging (MRI) of the brain with and without contrast was performed, which revealed evidence of neuro-sarcoidosis based on hypothalamic and leptomeningeal enhancement. Due to these manifestations, it was recommended to start oral prednisone and undergo bronchoscopy to try and obtain tissue to confirm the sarcoid diagnosis. Systemic sarcoidosis was confirmed via lung biopsy due to the presence of granulomas consisting of epithelioid cells and he was started on 80 mg/day and subsequently tapered to 40 mg/day, 20 mg/day,10 mg/day, and 1 mg/day over the course of 4 months. A repeat MRI was performed three months after starting oral prednisone which showed marked improvement of the previously described enhancement within the hypothalamus and superficial leptomeningeal regions. The patient developed side effects from the high doses of oral steroid, mainly puffiness of feet, abdominal bloating, and weight gain. Ultimately, the patient was placed on long-term immunosuppressive therapy with the Disease-modifying antirheumatic drug (DMARD) of methotrexate with the goal of decreasing the recurrence of neuro-sarcoid. He continues to monitor with us in optometry every six months and concurrently co-managed with neurology, pulmonology, cardiology, and primary care.
Discussion
1. Systemic sarcoidosis
Sarcoidosis is an inflammatory condition with an unclear etiology. It is suspected that the disorder involves an abnormal immune response directed against various unknown antigens.3 Infectious triggers such as mycobacteria along with genetic and environmental influences have been suspected to play a role in the pathogenesis of the disease.3 A complex cellular response to the antigen results in the formation of non-caseating granulomas in multiple organ systems.3 These granulomas consist primarily of epithelioid cells, multinucleated giant cells, and CD4+ T cells.3
The incidence of sarcoidosis varies based on geographic area and ethnicity. In the United States, sarcoidosis has an incidence of 35.5 per 100,000 in African Americans compared to 10.9 per 100,000 in Caucasians.4 The lungs are the main organs affected, prevalent in 90% of patients.5 The most common organ systems affected outside of the lungs are the skin, eyes, and heart. Extrapulmonary disease may manifest before, at the same time as, or after pulmonary disease.5 Patients may be asymptomatic or exhibit symptoms such as fever, malaise, or weight loss.
Patients demonstrating involvement of the CNS are said to have neuro-sarcoidosis, which is found in 5-13% of cases.6 Neuro-sarcoidosis can affect intracranial structures, such as the leptomeninges and hypothalamus, cranial nerves, and spinal cord.6 As it commonly masquerades as other conditions, diagnosis can be difficult and typically requires neuro-imaging and/or cerebrospinal fluid analysis.7 Oral corticosteroids are the first line of treatment for neuro-sarcoidosis, with intravenous usage in more severe cases.6 Following a steroid taper many patients may relapse, thus necessitating the use of immunosuppressive agents as a second-line therapy as portrayed in this case.8
2. Ocular sarcoidosis: Frequency, incidence, prevalence
The eye is affected in approximately 30-60% of people with sarcoidosis, with uveitis being the most common ocular manifestation.1 A study by Rothova et al in 1989 showed that uveitis preceded the non-ocular signs of sarcoidosis in approximately 30% of cases.2 The frequency of ocular manifestations of sarcoidosis varies based on geographic area, with ocular sarcoidosis being more prevalent in Japanese case studies compared to American and European studies. Age distribution of ocular sarcoidosis is bimodal, with peak incidences at 20-30 years and 50-60 years.3 In America, the prevalence of ocular sarcoidosis is greater in African Americans than Caucasians. Furthermore, African Americans tend to develop uveitis at an earlier age than Caucasians (35-44 years old compared to 43-52 years old).4
There is a wide spectrum of ocular manifestations of sarcoidosis (Table 1). Any part of the eye and adnexa can be involved either in isolation, or simultaneously. The lacrimal gland is the most affected adnexal tissue.9 Granuloma formation in the lacrimal gland can progress to cause severe keratoconjunctivitis sicca, or may spontaneously resolve, as in the case of the patient described in this case.
3. Uveitis and sarcoid associated uveitis
Sarcoid related uveitis is typically bilateral and approximately 90% become chronic.10 It can present as anterior, intermediate, posterior, or pan-uveitis; making it a possible differential of almost any presentation of uveitis. While sarcoid related uveitis is typically categorized as granulomatous, those with an early onset of disease or less severe inflammation can present with non-granulomatous uveitis. Common symptoms of anterior uveitis are eye pain, redness, photophobia, and decreased vision. This patient presented with decreased vision and a pressure sensation behind his left eye which presented with greater inflammation. Eye pain or a sensation of pressure can be caused by ciliary spasm or an elevated IOP.10 IOP elevation can be due to an obstruction of trabecular meshwork by a large number of inflammatory leukocytes, trabecular meshwork nodules/inflammation, and/or PAS.10 The presence of trabecular meshwork nodules and PAS can only be determined by performing gonioscopy.
4. Diagnostic criteria of ocular sarcoidosis
Diagnostic criteria for sarcoidosis-related uveitis have been outlined by the first IWOS in 2009.11 The criteria are based on intraocular signs suggestive for the diagnosis of ocular sarcoidosis and investigational tests supportive of the diagnosis of ocular sarcoidosis. A biopsy proving the presence of non-caseating epithelioid cell granulomas is required to confirm the diagnosis of sarcoidosis.11 The IWOS outlines criteria that must be met for the diagnosis of presumed, probable, and possible ocular sarcoidosis, in cases where a biopsy is not able to be performed. The patient initially fit the category of presumed ocular sarcoidosis since he had a “compatible uveitis” due to the presence of bilateral inflammation, bilateral hilar adenopathy on chest X-ray, and did not have a lung biopsy. After the lung biopsy confirmed the presence of non-caseating epithelioid cell granulomas, he fit into the category of definite ocular sarcoidosis.
Few studies have been conducted to validate the diagnostic criteria proposed by the 2009 IWOS. In 2017, Acharya et al. conducted a multicenter retrospective medical record review and investigated the sensitivity and specificity of the IWOS clinical signs and laboratory tests for diagnosing ocular sarcoidosis in an international population.12 They found that no one clinical sign was sensitive in the diagnosis of ocular sarcoidosis.13 In fact, 10% of patients with biopsy-proven sarcoidosis showed either no clinical signs or only had bilaterality.13 Furthermore, the only investigational test that was sensitive alone was bilateral hilar lymphadenopathy on chest radiograph, which was sensitive in 81% of biopsy-proven patients.13
5. Diagnostic criteria for systemic sarcoidosis: Imaging and laboratory testing
Clinicians often think to order serum ACE and serum lysozyme when suspicious of sarcoidosis. ACE is representative of total granuloma burden on the body and large fluctuations in ACE levels are prevalent in sarcoidosis.3 Certain medications can also affect ACE levels and it is important to take the patients systemic health and medications into account when interpreting ACE values. For example, in this patient, his serum ACE level was 69 U/L in October 2015 during the time he had bilateral lacrimal gland infiltration, which then normalized to 65 U/L in February 2018 during his first episode of active anterior uveitis. When the anterior uveitis recurred and bloodwork was repeated, his serum ACE level was 68 U/L. The reference range for ACE is between 9-67 U/L, indicating that the patient was at the high range of normal during his first active uveitis episode. This illustrates the ability of ACE to fluctuate during sarcoidosis and that normal serum ACE levels do not exclude the diagnosis of sarcoidosis, especially in cases of isolated ocular sarcoidosis. Additionally, for sarcoidosis associated uveitis, there is no association between uveitis activity and serum ACE levels.12 New research investigating alternative diagnostic biomarkers of sarcoidosis in patients with uveitis suggests poor sensitivity and specificity of serum ACE and lysozyme. A retrospective study by Jones et al. correlated significant lymphopenia (<1.0 x 109/l) with sarcoidosis in new patients with uveitis related to sarcoidosis compared to controls.14 Additionally, Gundlach et al. proposed that serum soluble interleukin-2 receptors (sIL2R), a marker for T cell activation which plays a role in inflammation, may be a more useful marker of the disease, as these levels are elevated in sarcoidosis patients with extrapulmonary involvement.15
A chest X-ray is a common screening tool for the diagnosis of sarcoidosis since most patients will have pulmonary involvement (90%). The finding of bilateral hilar lymphadenopathy is highly suggestive of sarcoidosis but may also be present in other diseases such as tuberculosis and fungal infections. Recent development in imaging has led to the use of chest computed tomography (CT), positron emission tomography (PET) scan and gallium scintigraphy to aid in the diagnosis of sarcoidosis when chest X-ray results are unclear. This patient showed bilateral hilar lymphadenopathy (Figure 2).


The most sensitive test for confirming the diagnosis of sarcoidosis is a biopsy of suspicious tissue.5 Common biopsy sites include the lungs, lymph nodes, skin, and conjunctiva.5 Due to the invasive nature of biopsies, they are typically not performed in asymptomatic patients with minimal signs. In the case of our patient, a transbronchial lung biopsy was recommended only after the patient developed constitutional symptoms and neuroimaging was performed which showed CNS manifestations.
6. Complications of ocular sarcoidosis
Short term/immediate visual impairment from sarcoid related uveitis may be due to a prescription shift and/or blur from photosensitivity. This patient had a 1.50 D myopic shift in his left eye at the initial exam and was also symptomatic for blur on the computer screen at work due to the brightness of the screen. Chronic causes of visual impairment secondary to uveitis may be in the form of cataract formation, cystoid macular edema, and/or uveitic glaucoma. If the elevated IOP is due to the accumulation of inflammatory cells in the trabecular meshwork, then it is possible that the IOP will decrease as the inflammation resolves. Typically, patients are placed on temporary anti-ocular hypertensive eye drops to prevent damage to the optic nerve while IOP is still high. Patients are treated with aqueous suppressants such as beta-blockers and carbonic anhydrase inhibitors. The use of prostaglandin analogs in patients with uveitis is controversial and was avoided in this patient.9 Cases where topical anti-ocular hypertensives alone are not effective in controlling IOP, surgical interventions may be needed. Multiple studies show that there is a higher rate of failure of tubes and trabeculectomies in uveitic glaucoma compared to primary open angle glaucoma.10 In general, sarcoid related uveitis has a good prognosis. In one retrospective study of biopsy-proven sarcoid related uveitis cases, the presence of cystoid macular edema and chronic ocular inflammation were associated with poor visual prognosis.11
7. Treatment and management of ocular sarcoidosis
The goal of treatment of sarcoid related uveitis is to control the inflammation to prevent permanent visual damage. Topical corticosteroids are the mainstay of treatment in anterior uveitis. High initial doses of prednisolone acetate 1% with slow tapering is effective in most cases. Difluprednate 0.05% can be considered as well. Severe cases of iritis, refractory to topical corticosteroids or with posterior involvement, may require regional corticosteroid injections (sub-conjunctival or intravitreal). Careful monitoring of IOP should be performed as corticosteroids may cause IOP elevation.
Systemic corticosteroids are reserved for cases where severe bilateral uveitis is uncontrolled with topical or regional therapy. Systemic immunosuppressants and biologics have also been proven to be effective in treating uveitis, however management with the patient’s primary care provider should be done before initiating this therapy.16 This patient was started on systemic corticosteroids and ultimately managed with DMARDs due to his CNS manifestations of sarcoidosis.
Conclusion
Sarcoidosis is an inflammatory condition which predominantly affects the lungs but may have extrapulmonary manifestations. In some cases, it is the manifestation of ocular signs which leads to the diagnosis of sarcoidosis. Uveitis is the most common ocular manifestation and can be sight threatening, especially in chronic cases. Diagnosis remains difficult since biopsies are not routinely performed and many laboratory tests such as serum ACE and lysozyme have low specificity and sensitivity. For this reason, some cases of idiopathic uveitis may be later attributed to undiagnosed sarcoidosis. An inter-disciplinary approach to managing this condition is the only way to ensure proper care of these patients and prevent systemic and ocular complications of this multi-faceted disease.