INTRODUCTION
There has been limited literature published on the presence of transient corneal subepithelial cyst-like changes related to scleral lens wear,1,2 including a case series on macrocysts in corneas post-penetrating keratoplasty.3 Using spectral domain anterior segment optical coherence tomography (SD AS-OCT), this series highlights the presence and transitory nature of this benign finding in various conditions such as dry eye, post-radial keratotomy, and post-superficial keratectomy. These cases further support the theory that altered corneal physiology and anatomy, whether from surgery or disease, contribute to the formation of the subepithelial macrocysts with scleral lens wear. All patients remained asymptomatic and no macrocyst rupture or consequential corneal damage was observed.
CASE 1
A 77-year-old man presented to our clinic to be fit for specialty contact lenses due to severe dry eye disease (DED). Over the past six years, the patient had exhausted his dry eye treatment options, which included warm compresses, lid scrubs, artificial tears, lubricating ointment, cyclosporine 0.05% ophthalmic emulsion, fish oil capsules, oral doxycycline 100 mg per day, and punctal plugs. He also had three prior evaluations with corneal specialists; however, he still suffered from dry eye symptoms. The etiology of his dry eye was multifactorial, including meibomitis, blepharitis, and ocular rosacea. His current ocular medications included carboxymethylcellulose sodium 1.0% lubricant ophthalmic gel four times a day in each eye and cyclosporine 0.05% ophthalmic emulsion twice a day in each eye.
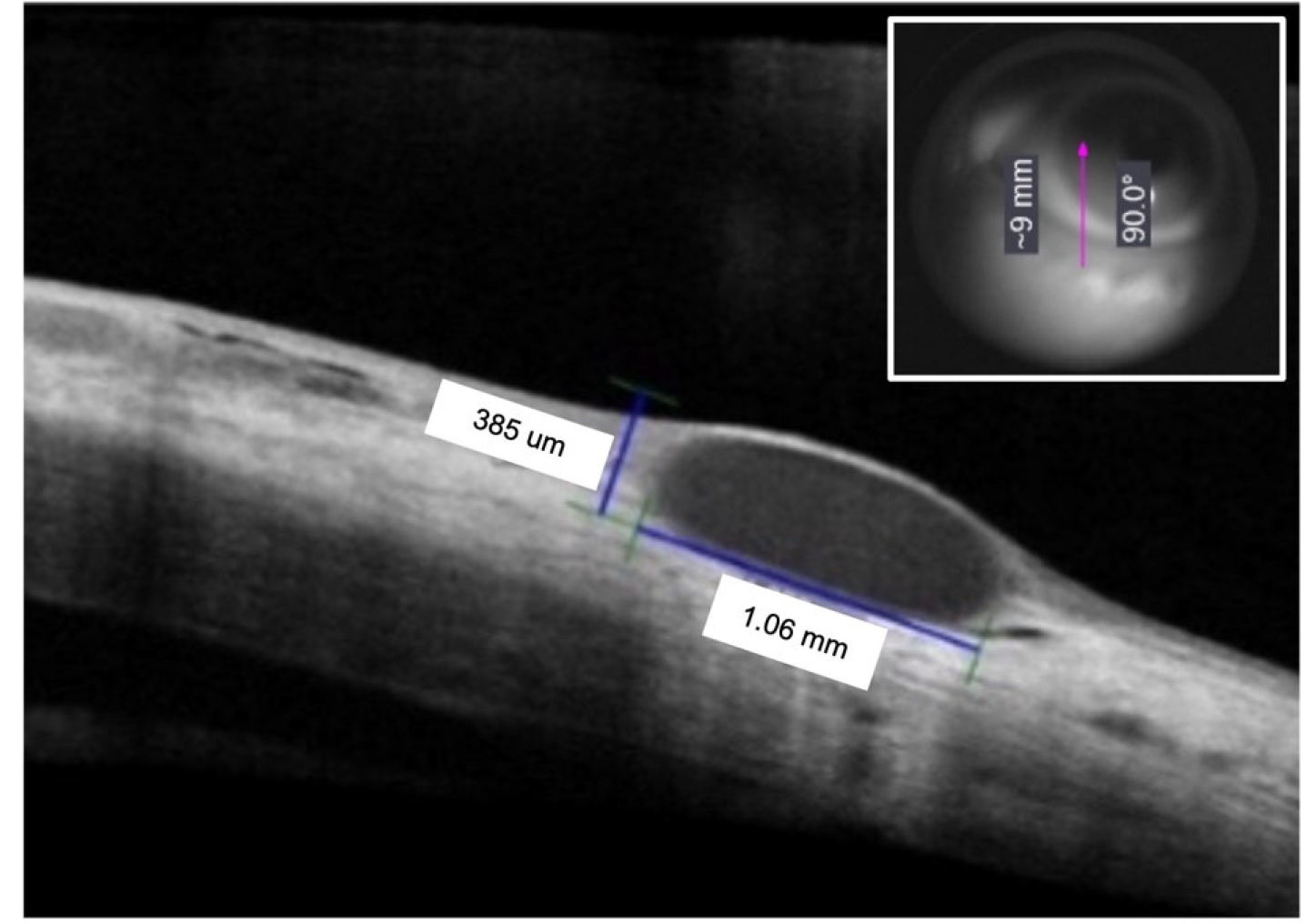
His best corrected visual acuity was 20/20-1 in the right eye and 20/25+2 in the left eye with pertinent ocular history of mild cataracts and extramacular drusen in both eyes. With the initial trial of a 18.2 mm full scleral contact lens on both eyes, corneal subepithelial macrocysts were noted at the temporal and superior limbus in areas of pannus and mild corneal edema in the right eye and nasal and superior in the left eye. These superficial macrocysts ranged from 1mm to 3mm in diameter. Spectral domain AS-OCT confirmed the location of the macrocysts as subepithelial (Figure 1). The patient denied any pain, discomfort, or photophobia. Removal of the lens resulted in resolution of the macrocysts within minutes.

Due to poor centration of the full scleral lens, a 15.6 mm mini-scleral lens was trialed on both eyes. No macrocysts were evident with the 15.6 mm mini-scleral lens. After several visits to modify lens parameters to improve fit, the final lens ordered was a 16.8 mm mini-scleral contact lens.
The amount of central clearance was assessed by comparison of the fluid reservoir beneath the scleral lens to the corneal thickness. Slit-lamp biomicroscopy revealed a fit with 1:1 central clearance, edge to edge limbal clearance and a slight inferior lens decentration. Visual acuity with the contact lenses was 20/20-1 OD and 20/25 OS. The patient reported marked improvement of dry eye symptoms. The transient corneal subepithelial macrocysts were observed in the same general location in the corneas while wearing the 16.8 mm mini-scleral lenses at every visit over the next four years without complications or symptoms.
CASE 2
A 67-year-old male presented for a contact lens fit for his right eye. Past ocular history included cryopexy, pars plana vitrectomy, and lensectomy of the right eye with an anterior chamber intraocular lens implant after sustaining blunt trauma with lens dislocation, iridodialysis and vitreous hemorrhage. Post-operatively, the right cornea was irregular after development of pseudophakic bullous keratopathy with microcystic edema and central corneal keloids. The right eye had central geographic atrophy with drusen and a central epiretinal membrane. The left eye had a mild age-related cataract. Subsequently, he had superficial keratectomy of the right cornea which resulted in diffuse stromal haze. This was speculated to be related to limbal stem cell deficiency (LSCD) from multiple surgeries.
His best corrected visual acuity with spectacles was hand motion in the right eye and 20/20 in the left eye. The right eye visual acuity improved to finger counting with a trial 15.6 mm mini-scleral lens. The amount of central clearance was assessed by comparison of the fluid reservoir beneath the scleral lens to the corneal thickness. Slit lamp evaluation of the lens fit revealed 0.75:1 central clearance and slight inferior decentration. The right cornea had approximately 1.5mm of neovascularization from the limbus 360 degrees with diffuse corneal haze and a thickened irregular epithelial surface. The left cornea was clear.
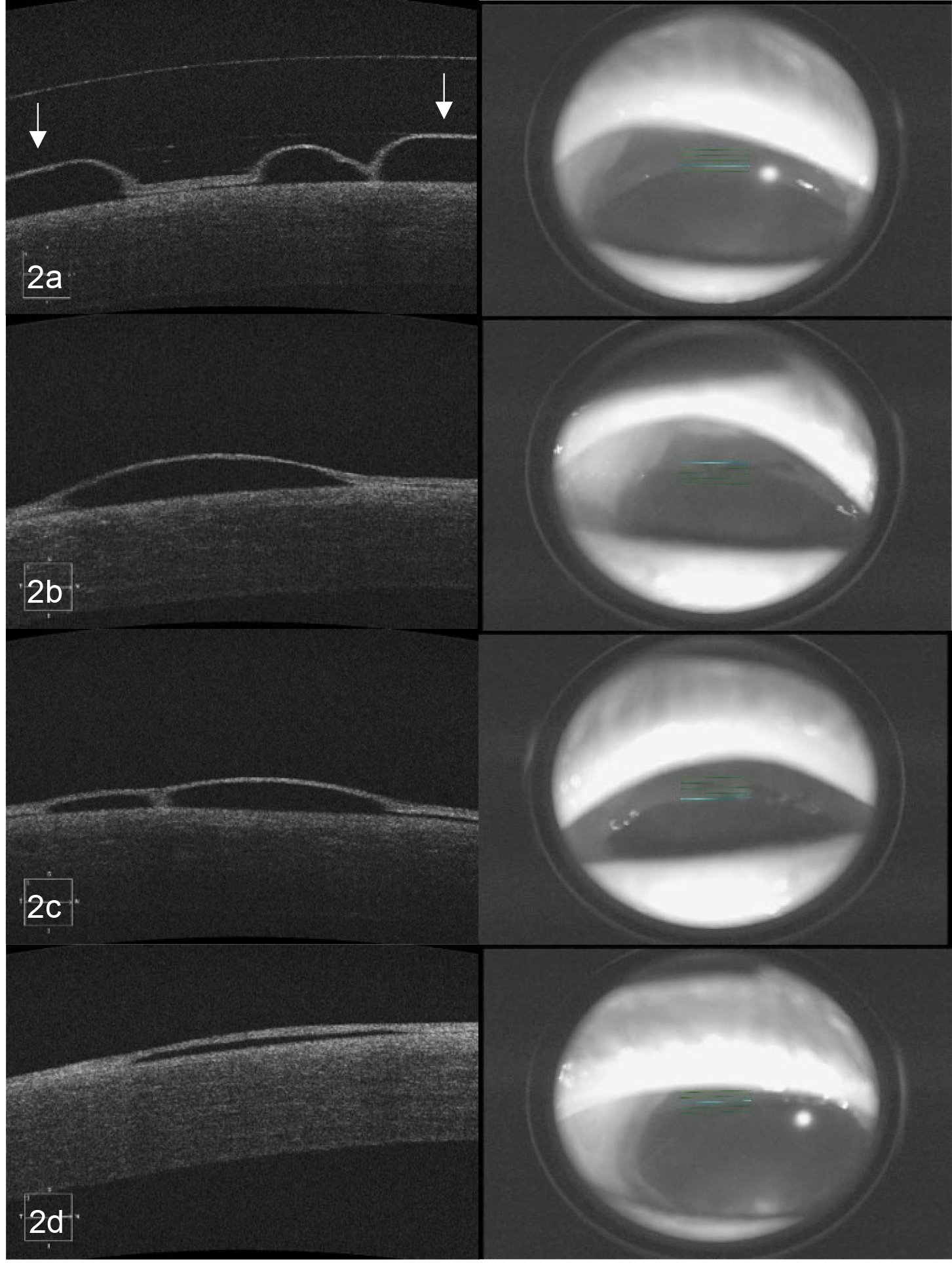
Multiple large corneal macrocysts were observed in the inferotemporal periphery during slit lamp evaluation of the right cornea. Spectral domain AS-OCT confirmed the location of the macrocysts to be subepithelial and multiple scans post-insertion and post-removal of the mini-scleral lenses were obtained to demonstrate their transitory nature (Figure 2). In comparison to the AS-OCT scan thirty minutes post-insertion, there was a significant decrease in the macrocysts’ size at five minutes post-removal. By ten minutes post-removal, the macrocysts were nearly resolved. The patient denied any symptoms such as pain, discomfort or photophobia.

CASE 3
A 68-year-old male presented for a contact lens fitting due to corneal scarring and irregular astigmatism status post radial keratotomy (RK), astigmatic keratotomy (AK), and laser in-situ keratomileusis (LASIK) of both eyes. His best corrected visual acuity with spectacles was 20/60 in the right eye and 20/40 in the left eye. With scleral contact lenses, he was able to achieve a visual acuity of 20/40 in the right eye and 20/25 in the left eye.
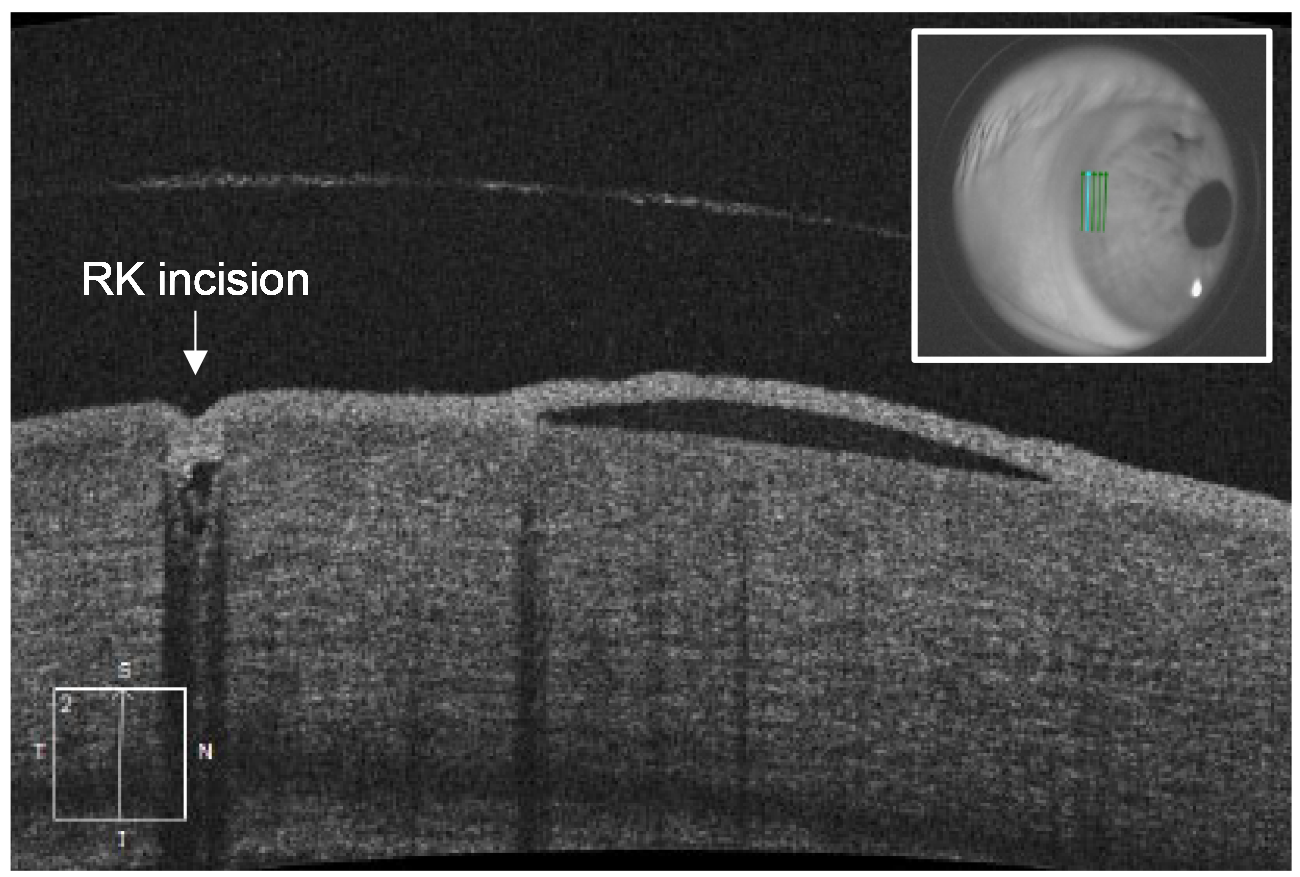
Slit lamp biomicroscopy revealed faint LASIK scars in both eyes, 11 RK scars with 4 AK scars in the right eye, and 8 RK scars with 6 AK scars in the left eye. Both corneas had mild neovascularization from 10:00 to 2:00 and extensive neovascularization along the RK scars. Two limbal superficial corneal macrocysts at 8:30 and 9:30 near incisional scars of the right cornea were observed while the patient was wearing Jupiter 15.6mm mini-scleral lenses. Spectral domain AS-OCT confirmed the location of the macrocysts to be subepithelial (Figure 3). No macrocysts were seen in the left eye.

The amount of central clearance was assessed by comparison of the fluid reservoir beneath the scleral lens to the corneal thickness. Slit lamp evaluation of the lens fit revealed 1:1 central clearance. After several visits to modify lens parameters to improve fit, the final lens ordered was a 17.0 mm reverse geometry mini-scleral contact lens.
With these lenses on, two subepithelial macrocysts were appreciated again at 9:30 in the right eye. Two smaller subepithelial macrocysts at 7:30 were also noted in the left eye. The macrocysts resolved 25 minutes after scleral lens removal. When the lenses were reinserted, the macrocysts formed after 30 minutes of wear. Throughout the follow ups over several months, the patient denied any symptoms such as pain, discomfort or photophobia. No rupture of the macrocysts or damage to the cornea was observed.
DISCUSSION
Transient corneal macrocysts are subepithelial collections of fluid that typically range from 0.5 to 2.0 mm in size. In this case series, each patient was observed with scleral lens wear on eyes with compromised epithelial attachment complexes due to various conditions such as trauma from severe dry eye disease or secondary to corneal surgery.
Dry eye disease (DED) is an ocular condition involving an inadequate or abnormal tear film and inflammation. The first patient case is an example of how challenging managing DED can be due to the multitude of factors which can affect the ocular surface and eyelids, such as the presence of rosacea. Rosacea is associated with ocular surface inflammation which disrupts tear film homeostasis and exacerbates evaporative dry eye disease.4
In eyes with a stable tear film, the corneal epithelial barrier is maintained by tight junctions between apical cells of the stratified epithelium. In dry eye disease, increased sodium ions cause osmotic stress – activating inflammatory cytokines, chemokines and matrix metalloproteinases.5 These inflammatory mediators in the tears lyse tight junction proteins and trigger apoptosis of the apical corneal epithelium and conjunctival goblet cells.5 This barrier disruption can result in epithelial defects and corneal edema.6,7 Corneal edema can also occur with pannus formation, which is frequently observed in late stages of severe dry eye disease.8,9 Our first patient had transient macrocysts form in focal areas of pannus and edema as areas of corneal edema have been found to have reduced epithelial adhesion.10
Corneal surgeries can also lead to poor epithelial attachments due to mechanical damage and corneal denervation. In the second patient case, superficial keratectomy was used to treat corneal keloids. Superficial keratectomy (SK) involves manual dissection of the superficial corneal layers by a blade or diamond burr. Other indications for SK include, but are not limited to, epithelial basement membrane dystrophy, Salzmann nodular degeneration, band keratopathy, recurrent corneal erosions, and suspected ocular surface neoplasia.11
The third patient with macrocysts had RK and AK performed on both eyes. Many RK and AK patients experience poor vision from irregular astigmatism, changes in corneal shape, and tear film instability. In cases where RK results in a highly irregular corneal surface, optical correction with scleral contact lenses is superior to spectacles, soft lenses or corneal rigid lenses. Scleral lenses can vault over an oblate anterior cornea while the fluid reservoir provides corneal hydration, resulting in stable and clearer vision.12 However, clinicians should also be aware of possible complications when fitting RK patients with scleral lenses.
A small case study of five patients found that scleral lenses induced corneal edema in nine post-RK eyes.13 The edema was measured greatest in the midperiphery near the incision likely due to epithelial barrier dysfunction leading to increased permeability.13 Another study has shown increased endothelial degeneration in elderly patients status post-RK.14 Corneal neovascularization which forms in response to the injury from ocular surgeries, such as RK, can also lead to edema and weakened epithelial attachments.10,15 These factors likely contributed to the formation of the transient macrocysts along the neovascularized RK incisions in our third patient case.
It is hypothesized that the transitory macrocysts form when negative pressure underneath the scleral lens displaces the loosely adhered epithelium.3 In all three cases, as well as in other previously reported cases of transient macrocysts with scleral lens wear, the cysts resolved within minutes after lens removal.1,3 In another similar report of corneal epithelial bullae after short-term wear of small diameter scleral lenses, all bullae resolved however the exact timespan for resolution was unknown.2
Since scleral-lens-induced transient macrocysts are seen in varying conditions, it is postulated that any disorder which considerably weakens the epithelial attachment complex may present with this finding. Therefore, it is probable that clinicians who regularly fit scleral lenses will eventually detect these subepithelial macrocysts. They can be easily missed without careful slit lamp evaluation of the midperipheral and peripheral cornea underneath the scleral lens. Anterior segment OCT can be used to confirm their subepithelial location.
CONCLUSION
Scleral lenses improve both vision and ocular surface condition in cases of corneal irregularity and ocular surface disease by creating a fluid reservoir which protects the cornea from inflammatory mediators in the tears while providing continuous lubrication.5,16 They are compatible with a fragile epithelium and comfortable for most patients to use.17 Clinicians should be aware that the conditions indicated for scleral lens wear may also predispose the cornea to formation of transient subepithelial macrocysts. As all cases have been asymptomatic, transitory, and without macrocyst rupture or consequent corneal damage, we conclude that their benign existence is not a contraindication to scleral lens wear.
Funding
The authors have no financial or proprietary interest in any material or method mentioned in this article. This article has been peer reviewed.