
Introduction
Purtscher’s retinopathy is a rare ocular condition that may be seen in patients with head trauma, chest compression injury, or long bone fractures, with annual incidence rates estimated to be 0.24 cases per million of the population.1 The disease involves multi-level retinal ischemia and can present simultaneously with paracentral acute middle maculopathy (PAMM) resulting in central vision loss.
Case Presentation
A 21-year-old white male presented four weeks following a recent suicide attempt where he had jumped off a five story building and suffered a traumatic brain injury. His medical history was unremarkable aside from recent trauma-related injuries including pulmonary contusion, right pneumothorax, left hemothorax, and bilateral rib and femur fractures.
Previous ocular history prior to the injury was unremarkable. He had visual acuities of 20/20 in both eyes with an emmetropic refraction, and all ocular health findings were normal in both eyes.
At his initial examination performed four weeks post-trauma, he complained of bilateral blurred and washed-out vision. Best corrected visual acuities were 20/100 in the right eye and 20/40 in the left eye. Extraocular motility and confrontation visual fields were normal and there was no relative afferent pupillary defect. All anterior segment findings were unremarkable in both eyes and intraocular pressures were normal and symmetric. Fundus examination of the right eye revealed a blunted foveal reflex, multiple cotton wool spots and Purtscher flecken that were more severe along the inferior vascular arcades, and intraretinal hemorrhages. In the left eye, the macula was flat and there were peripapillary cotton wool spots, multiple Purtscher flecken, and intraretinal hemorrhages. The optic nerves in both eyes were found to be found with no disc edema, hemorrhages, or pallor. The peripheral retina was normal in both eyes with no holes, breaks, or detachments. Based on the retinal findings, a diagnosis of Purtscher’s retinopathy was made in both eyes. Retinal imaging was unavailable at that time.
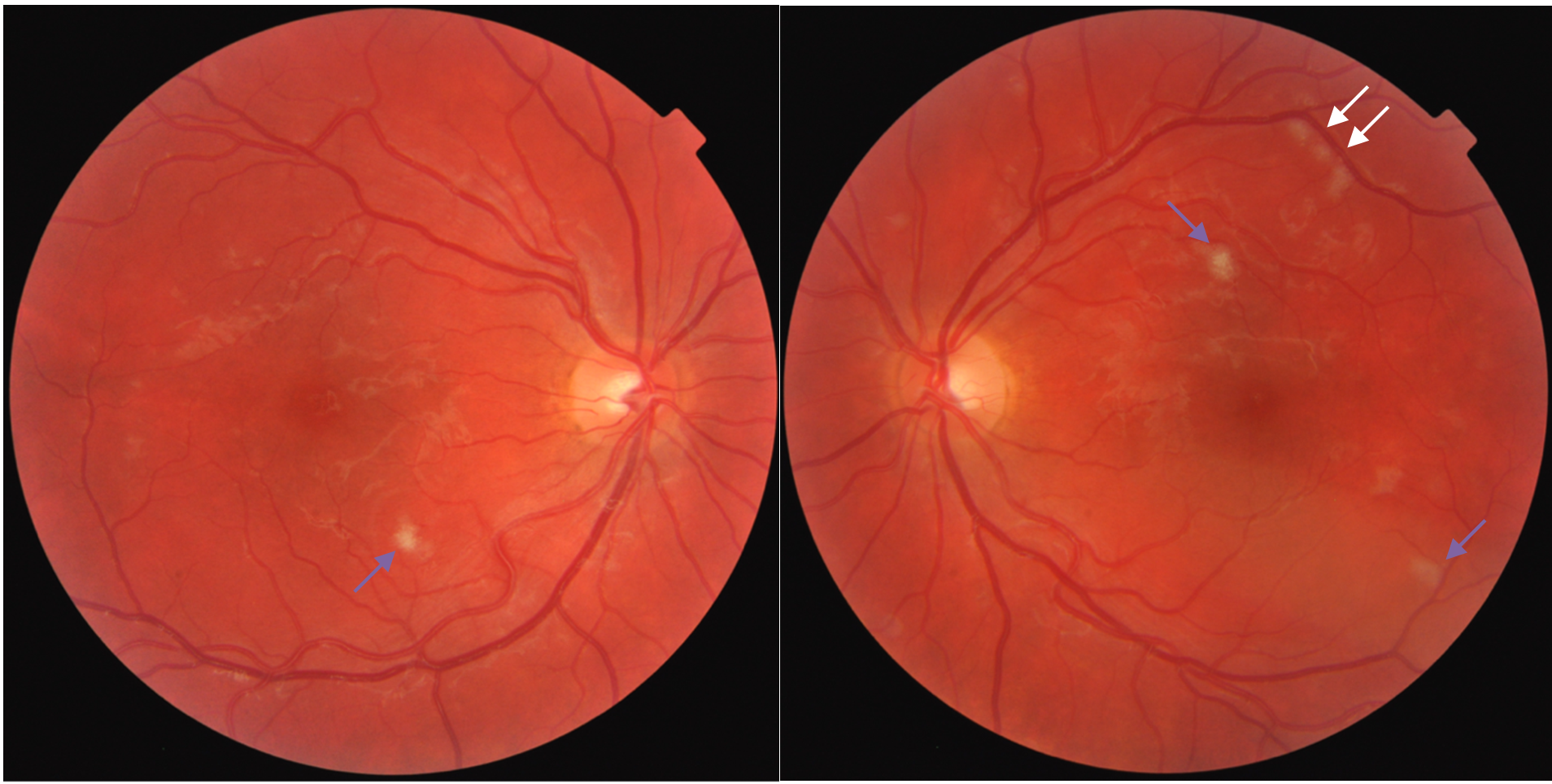
The patient was then transferred to a Polytrauma Rehabilitation Clinic and was evaluated six weeks post-trauma. Pinhole visual acuities at this visit were 20/100 in the right eye and 20/25 in the left eye. Entrance testing was stable. Anterior segment was unremarkable in both eyes and intraocular pressures were normal and symmetric. Gonioscopy revealed open angles and no angle recession in both eyes. Ophthalmoscopy revealed both optic nerves heads were flat, with no disc edema, hemorrhages, or pallor with positive foveal reflexes. Retinal findings included a single cotton wool spot in the right eye (Figure 1) and few cotton wool spots and Purtscher flecken in the left eye (Figure 1). No intraretinal hemorrhages were noted, and peripheral retina had no breaks, tears, or detachments in both eyes.
_and_left_eye_(right_image)_6_weeks_post-tr.png)
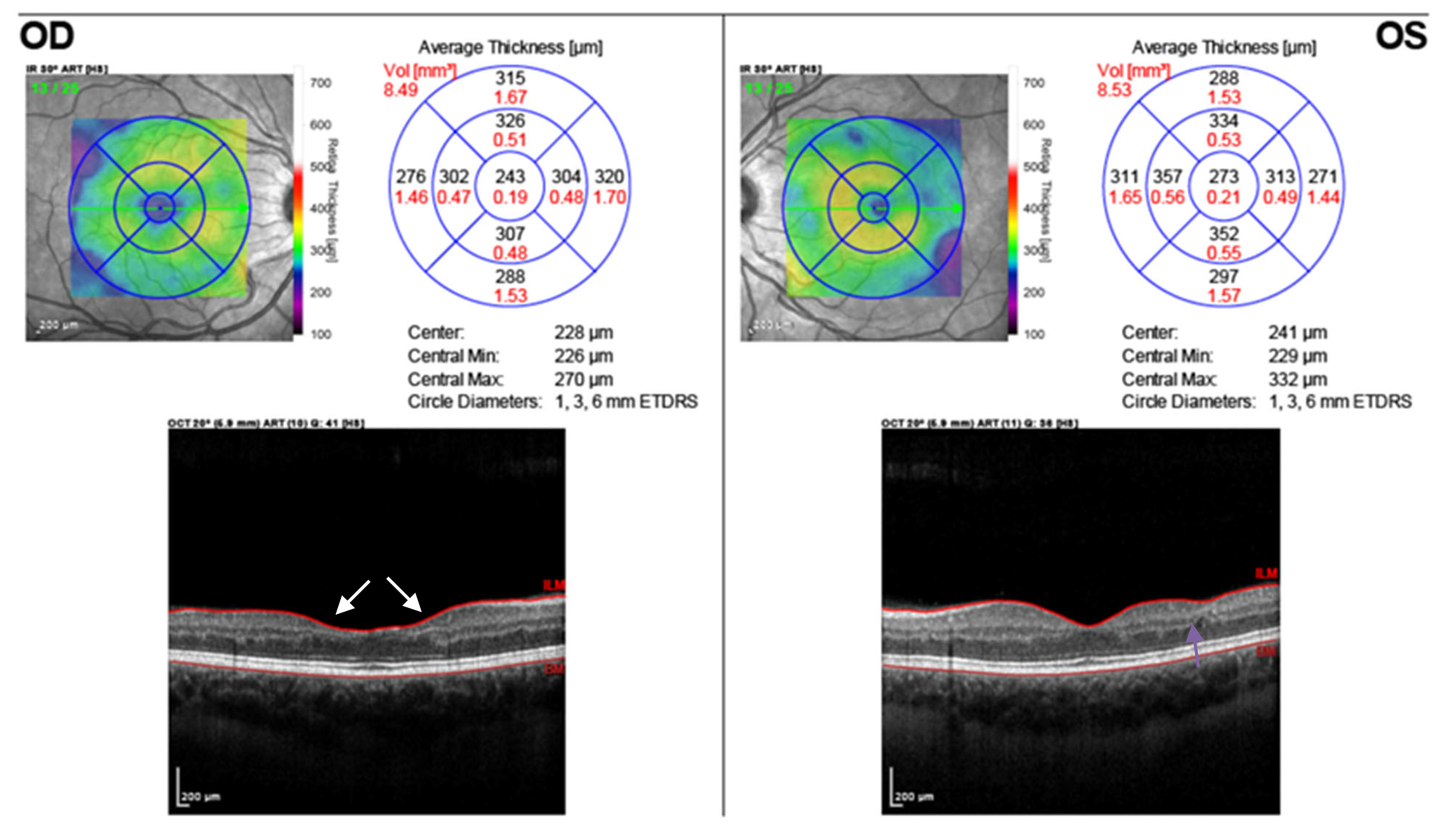
Cirrus spectral-domain optical coherence tomography (SD-OCT) v.9.5 (Cirrus OCT 5000, Carl Zeiss Meditec, Dublin, California, USA) of the right eye revealed good foveal contour, and the outer retinal layers, including the retinal pigment epithelium, interdigitation zone, and ellipsoid zone, were intact. There was a hyperreflective band-like lesion in the paracentral inner nuclear layer, consistent with PAMM (Figure 2A). This lesion was most prominent nasal, temporal, and inferior to the fovea. There were also focal areas of atrophy of the inner nuclear layer with mild collapse of the overlying superficial retinal layers superotemporal and temporal to the macula, indicating areas of chronic ischemia (Figure 2B). The left eye had good foveal contour on SD-OCT and outer retinal layers were intact. SD-OCT revealed a hyperreflective band-like lesion in the paracentral inner nuclear layer, consistent with PAMM (Figure 2C), and the lesion was most prominent superior to the fovea. There were more focal areas of atrophy of the inner nuclear layer superior and temporal to the macula (Figure 2D).
_and_left_eye_(c_d)_6_weeks_post-trauma.png)
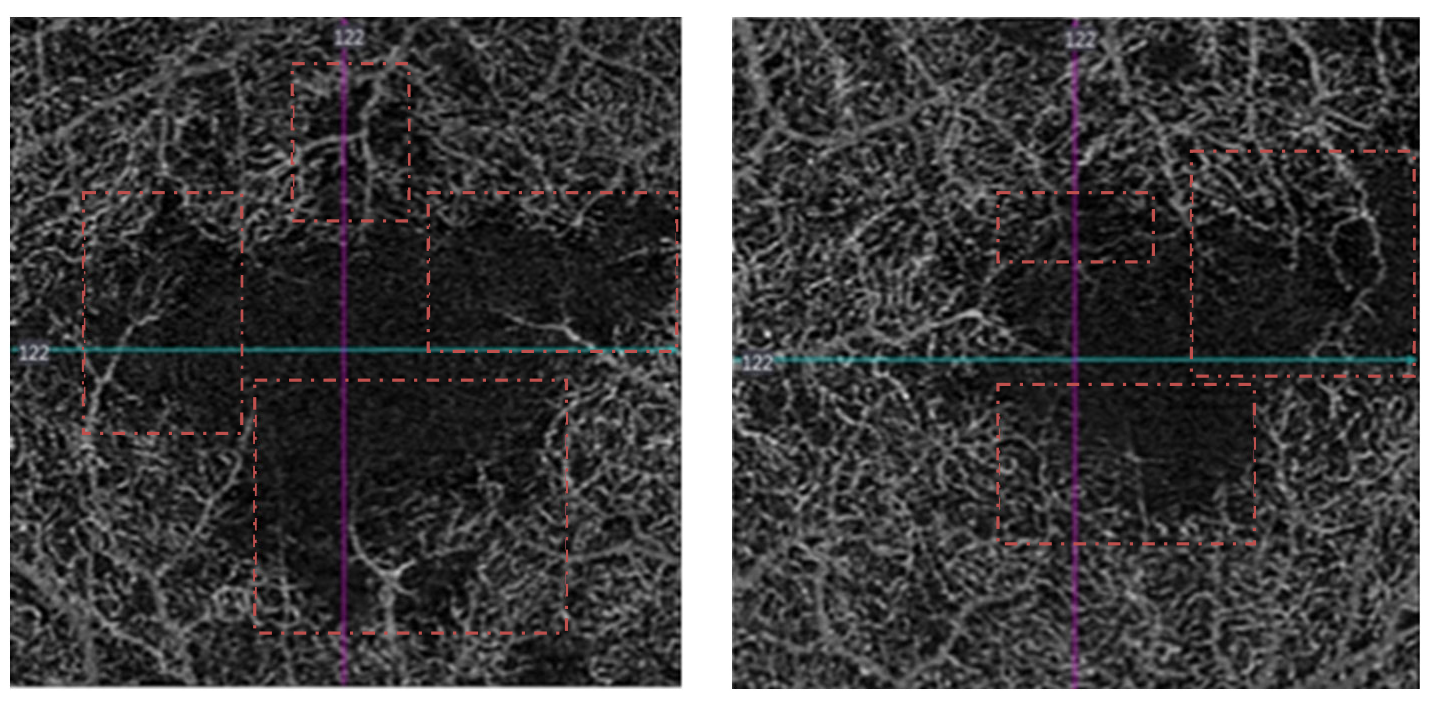
Cirrus optical coherence tomography angiography (Angioplex, Cirrus HD OCT 5000, Carl Zeiss Meditec, Dublin, California, USA) of the right eye revealed parafoveal dropout of deep retinal capillaries; most prominent nasal, temporal and inferior to the fovea indicating ischemia to the deep retinal capillary plexus (Figure 3), consistent with the location of the PAMM lesions. Optical coherence tomography angiography (OCTA) of the left eye revealed dropout of deep retinal capillaries most prominent superotemporal and inferior to the fovea (Figure 3) that corresponded with the inner nuclear layer atrophy noted on SD-OCT. Superficial retinal capillaries were largely intact in both eyes.
_and_left_eye_(right_image)_6_week.png)
The patient was seen for follow up and visual field testing eight weeks post-trauma. Pinhole visual acuities improved to 20/30 in the right eye and 20/20 in the left eye; significantly improved compared to his two prior examinations.
A baseline visual field 30-2 test using the Swedish Interactive Thresholding Algorithm (SITA) Standard strategy was completed with the Humphrey Field Analyzer 3 (Carl Zeiss Meditec, Dublin, CA, USA). Visual field testing revealed mild paracentral defects nasal, temporal, and superior to fixation in the right eye and shallow pericentral defects with three deep inferior and nasal focal defects in the left eye. The visual field defects were consistent with the location of the PAMM lesions on SD-OCT in the right eye and corresponded to an area of inner retinal atrophy superotemporal to the fovea in the left eye.
Due to his upcoming discharge from the clinic, it was recommended that the patient have a dilated eye exam in six months with updated macula OCT.
At a follow up 85 weeks post-trauma, the patient’s visual acuity remained mildly decreased at 20/40 in the right eye with 20/15 visual acuity in the left eye. Spectralis SD-OCT v.6.8.3 (Heidelberg Engineering, Heidelberg, Germany) of the right eye revealed irregular and enlarged foveal contour due to atrophy of the parafoveal inner nuclear layer corresponding to the previously seen hyperreflective band within the inner nuclear layer (Figure 4). Previously noted areas of focal inner nuclear layer atrophy superotemporal to the fovea in the right eye were stable. Outer retinal layers, including the retinal pigment epithelium, were intact in the right eye. SD-OCT of the left eye revealed normal foveal contour, but also revealed atrophy of the inner nuclear layer superior to the fovea corresponding to the previously seen hyperreflective band within the inner nuclear layer (Figure 2). Previously noted areas of focal inner layer atrophy temporal to the fovea were stable and outer retinal layers, including the retinal pigment epithelium, were intact in the left eye (Figure 4).
_spectralis_macular_sd-oct_of_the_right_eye_(left_image)_and_left_eye_(right_image)_85_.png)
Discussion
The hallmark of Purtscher’s retinopathy is the presence of Purtscher flecken, cotton wool spots, and intraretinal hemorrhages localized to the posterior pole. Flecken are characterized as polygonal areas of retinal whitening that are found between retinal arterioles and located deeper in the retina, compared to the superficial cotton wool spots. Additionally, flecken can be differentiated from cotton wool spots their distinct clear zone between the lesion and the arterioles, corresponding to the 50um capillary-free zone surrounding retinal arterioles.1–4 Purtscher’s retinopathy may also present with possible optic disc edema, although rare.5
Paracentral acute middle maculopathy is a novel finding on SD-OCT that had previously been undiagnosed largely due to the subtlety of retinal findings and lack of abnormalities on fluorescein angiography.2 Acute findings on SD-OCT will reveal a hyperreflective band-like lesion within the inner nuclear layer, with eventual atrophy of this layer in the chronic phases.2,5–8
Findings on OCTA will typically reveal abnormalities of the deep retinal capillaries with dropout of the capillary bed adjacent to the foveal avascular zone, corresponding to the paracentral location of the PAMM lesions.2,9,10 Although retinal findings are not necessary for diagnosis, when present, ophthalmoscopy will reveal muted gray lesions in the parafoveal region.11
To date, there has only been one other reported case report of PAMM associated with Purtscher’s retinopathy in a patient who suffered long bone fractures.3 This is the first case report, to our knowledge, of a patient with Purtscher’s retinopathy who suffered traumatic brain injury, chest compression, and long bone fractures who also had a concurrent finding of bilateral PAMM.
It has been recognized that Purtscher’s retinopathy occurs due to occlusion of the precapillary retinal arterioles due to trauma-induced emboli. The specific emboli can vary depending on the nature of injury, with air emboli likely being the cause in cases of traumatic brain injuries and chest compression injuries.6–8 In cases that result from bone fracture, fat or fibrin emboli may be more likely culprits.3 However, in our case, the cause of Purtscher’s retinopathy was likely multifactorial as our patient had suffered head trauma, pulmonary contusion, and bone fractures.
There are four retinal capillary networks within the posterior pole, and it is thought that the embolic occlusion of the precapillary arterioles results in multi-level retinal ischemia. The radial peripapillary capillary plexus lies within the retinal nerve fiber layer and has fewer anastomoses. Thus, occlusion of the arterioles supplying this capillary network can produce microinfarctions localized around the optic nerve, as is classic for Purtscher’s retinopathy.5,6 Ischemia to the superficial capillary plexus can result in superficial infarcts that are visualized as cotton wool spots.6 Deeper retinal layers are perfused by the intermediate and deep capillary plexus, which are supplied by the vertical anastomoses of the superficial capillary plexus. Thus, precapillary arteriole occlusion could potentially lead to further downstream ischemia to the deeper retinal capillaries and present clinically as Purtscher flecken.12
Considering the multi-level retinal ischemia in Purtscher’s retinopathy, it is possible to have concurrent PAMM in these patients, as PAMM represents deep capillary ischemia.2,13 The paracentral fovea is a watershed zone susceptible to retinal ischemia due to its high oxygen demand yet limitation on capillary density to maintain optimal optical light penetrance.9,14,15 Thus, this specific region of the retina is particularly vulnerable to ischemia and explains its association with many other retinal vascular diseases.
Both Purtscher flecken and PAMM represent deep capillary ischemia, however the location of the lesions will differ. Whereas Purtscher flecken are prominent in the peripapillary region, PAMM lesions will be concentrated in the foveal region, and may represent the same ischemic process.
Management and Outcomes
Initial visual acuity with Purtscher’s retinopathy can range from normal to hand motion. In a study by Agrawal and McKribbin, it was shown that there can be spontaneous recovery of at least two Snellen lines of visual acuity in half of the cases of Purtscher’s retinopathy, with chances for better visual recovery if the acute retinal findings had resolved within one month.1
Due to its’ association with many retinal vascular diseases such as diabetic retinopathy, hypertensive retinopathy, and vascular occlusions,4,12 it is difficult to predict visual prognosis in patients with PAMM, as prognosis varies depending on concurrent retinal diagnosis. However, in a case series of patients presenting with PAMM, without evidence of other retinal pathology, it was found that these patients had visual acuities ranging from 20/15 to 20/30 due to sparing of the central fovea; indicating a relatively good visual prognosis with PAMM alone. In the patients with mildly reduced best corrected visual acuity, visual acuity measurements tended to remain stable without improvement.14 This case report presents a unique case of a patient who suffered polytrauma and experienced significant improvement in visual acuity up to 8 weeks post-trauma, but had final visual acuity that remained reduced at 20/40 even at 85 weeks post-trauma.
There is currently no accepted treatment for either Purtscher’s retinopathy or PAMM. In a systematic review regarding the efficacy of glucocorticoid treatment for Purtscher’s retinopathy, it was determined there was no statistical significance between treated and non-treated patients.16 Given the high likelihood for spontaneous visual recovery with Purtscher’s retinopathy, it is recommended these patients be monitored, without treatment, for visual recovery. Although there is no treatment for PAMM, emphasis should be made to control underlying vascular pathology to prevent recurrence in patients with associated risk factors. Given that our patient’s diagnosis of PAMM was the result of polytrauma, no further management was indicated.
Similar to studies regarding visual recovery in patients with Purtscher’s retinopathy,7 our patient made significant visual recovery within the first eight weeks following his injury. However, visual acuity remained reduced at 85 weeks post-trauma, in contrast to a previous case report of a patient with PAMM and Purtscher’s retinopathy who had normal acuity.3 As seen on SD-OCT, our patient had significant atrophy of the middle parafoveal retina likely contributing to the reduced visual acuity (Figure 4).
In patients with Purtscher’s retinopathy, visual acuity can be expected to improve, however those with concurrent findings of PAMM should be educated that paracentral scotomas may persist due to atrophy of the middle parafoveal retina.
Conclusion
Purtscher’s retinopathy and PAMM are conditions associated with retinal ischemia. This case report demonstrates that both conditions can present concurrently in a polytrauma patient. Thus, it is important to consider PAMM as a cause of central or paracentral vision loss in a patient presenting with Purtscher’s retinopathy.
CE Notification
This article is available as a COPE accredited CE course. You may take this course for 1-hour credit. Read the article and take the qualifying test to earn your credit. [CLICK HERE TO ENROLL]
Please check COPE course expiry date prior to enrollment. The COPE course test must be taken before the course expiry date.