Introduction
Treponema pallidum causes syphilis via direct sexual exposure, through the placenta during any gestational period, or through vertical transmission as the unborn child touches the maternal genital lesions in the birth canal.1 A spirochete, T. pallidum, causes local inflammatory reactions by traveling and replicating throughout the body.2 If it penetrates the blood-brain barrier, T. pallidum causes neurosyphilis.2 The Centers for Disease Control and Prevention (CDC) defines ocular syphilis as clinical symptoms or signs consistent with ocular disease with syphilis of any stage.3–5 All cases of syphilis must be reported to local departments of health (DOH), which aids in identifying, testing and treating all involved partners.2 In this paper, we present a case of a progressive bilateral granulomatous panuveitis secondary to syphilis.
Case Presentation
A 60-year-old male presented with complaints of blurred vision and black and white spots in the temporal field in both eyes. He also noted redness in both eyes beginning three months prior to presentation. His past ocular history was remarkable for migraines with aura. His medical history was remarkable for hearing loss and tinnitus, coronary stent, hypertension, and non-alcoholic fatty liver. He was being evaluated for non-tuberculous mycobacterial lung infection with multiple lung nodules. His medications included tamsulosin, hydrochlorothiazide/losartan, aspirin 81mg, atorvastatin, and metoprolol.
On examination, the patient had a best-corrected visual acuity (VA) of 20/20 in each eye. Pupils, extraocular muscle motilities and confrontation fields were unremarkable. Anterior segment of both eyes revealed 2+ diffuse bulbar conjunctival injection, 2+ diffuse fine and mutton fat keratic precipitates (KPs) with mild corneal edema centrally, and 1+ cells with 1+ flare in the anterior chamber of each eye. A Koeppe nodule was noted at 12 o’clock on the right iris. Intraocular pressure was 10mmHg and 12mmHg for the right and left eye, respectively. A dilated fundus exam was unremarkable in both eyes. The patient was diagnosed with chronic granulomatous anterior uveitis in both eyes and was prescribed difluprednate 0.05% ophthalmic emulsion four times a day in both eyes. Follow up visits on day three and week two revealed improving signs and symptoms.
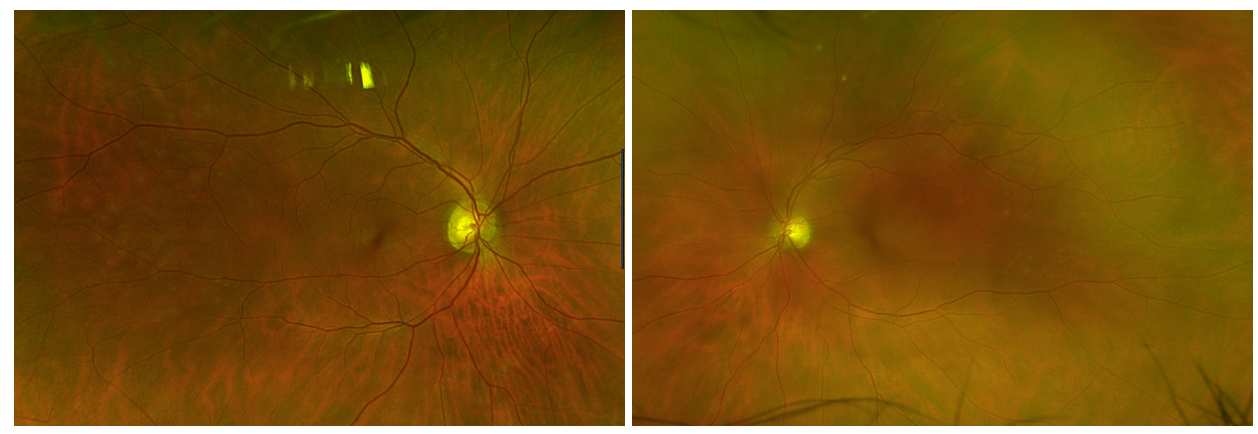
One month later, the patient presented with new complaints of a headache above the brow with pressure in and around both eyes that had developed the night before. He stated the pressure persisted that night and he could not open his eyes. The next morning the pain had resolved but his vision became “cloudy”, and the bilateral conjunctival redness had returned. His VA was 20/25-2 in the right eye and 20/25 in the left eye. Pupils were equal and round without an afferent pupillary defect however there was now a sluggish pupillary response in both eyes. Anterior segment revealed 1+ diffuse bulbar injection in both eyes with mutton fat KPs and fine KPs with trace punctate corneal epithelial erosions left eye greater than right eye. There were 2+ cells in the anterior chamber of each eye with fibrin strands in the left eye. Intraocular pressures were 22mmHg in the right eye and 21mmHg in the left eye. Dilated fundus examination revealed trace cells in the anterior vitreous of both eyes along with posterior vitreous cells in the left eye. There were patches of retinal whitening in the temporal midperiphery of each eye (Image 1). The patient was diagnosed with a recurrent bilateral uveitis with progression to a panuveitis and referred to ophthalmology.

A fluorescein angiogram was performed and confirmed an inflammatory lesion superior temporal in the left eye without papillitis, cystoid macular edema or vasculitis in either eye. Laboratory testing revealed reactive syphilis labs; sarcoidosis, tuberculosis, and Lyme disease all revealed negative results. The patient was referred to the infectious disease service; the patient was subsequently diagnosed with neurosyphilis and treated with a fourteen-day course of continuous intravenous penicillin. He was instructed to restart the difluprednate four times a day in each eye; the panuveitis resolved in each eye by week four, with resulting VA of 20/20 in each eye.
Discussion
This case underscores the importance of obtaining a detailed history in patients who present with uveitis and reviewing the history again if a patient’s clinical course fails to improve or worsens with current therapy. It also emphasizes the need for increased vigilance with respect to syphilis–“the great imitator” –given its variety of clinical presentations and the rising number of cases over the past decade in the US.2,3 Signs of acquired syphilis include interstitial keratitis, intermediate uveitis, retinal vasculitis, optic neuritis, chorioretinitis, placoid chorioretinitis, and Argyll Robertson pupil.6 Collaboration with infectious disease specialist managing patients with syphilis is critical.
When the patient’s uveitis progressed, we realized that our initial history was incomplete (Table I). Further questioning revealed that that patient had presented to his local emergency department three months previously with a rash on his back and ankle swelling that started at the same time as the ocular redness. At that time, it was decided that his anti-hypertensive medication needed to be adjusted to resolve the ankle swelling; the rash was not further investigated nor explained. During secondary syphilis, a skin rash is often observed.2 This information and the patient’s clinical course led to FTA-ABS and PRP/VDRL testing for syphilis. Subsequent consultation with infectious disease directed the systematic treatment.
Our patient presented with a progressive granulomatous uveitis. Posterior uveitis and panuveitis are the most common presentations of ocular syphilis.3–5 Other common systemic causes of panuveveitis such as sarcoidosis and toxoplasmosis must be ruled out.4 Syphilitic uveitis accounts for an estimated 0.5 to 0.65% of uveitis cases and may occur during any stage of syphilis infection.5 The presenting symptoms depend on the ocular structure involved with decreased visual acuity as the most common chief complaint.4,5,7 Ocular manifestations may be unilateral or bilateral.8 Panuveitis due to syphilis can present with either a non-granulomatous or granulomatous anterior uveitis, have iris nodules, and be associated with increased intraocular pressure,5 as demonstrated in Table I.
Our patient continued to exhibit rebound inflammation until he completed the penicillin treatment. The recommended treatment for neurosyphilis is IV penicillin G for 10-14 days.4 Once syphilis it is appropriately treated, the secondary uveitis typically resolves with the judicious use of topical corticosteroids as adjunct therapy. The visual prognosis is generally good when antibiotic treatment is started promptly. If left untreated, approximately 25% of patients will have one or more systemic relapses in their lifetime; however, most remain in the latent stage.
The stages of syphilis are determined by clinical presentation2–4: primary syphilis presents with a chancre, a painless ulcer, at the site of infection; secondary syphilis with a fever, skin rash, mucocutaneous lesions, and lymphadenopathy; and tertiary syphilis with significant cardiac or neurological conditions, skin lesions or bony involvement. Latent syphilis is defined as positive serologic testing without any clinical manifestations.2,3 An estimated 30% of untreated syphilis patients go on to develop tertiary syphilis.2,4
Conclusion
All cases of bilateral, recurrent, or worsening uveitis require a thorough history and a low threshold for syphilis testing. As cases of syphilis are increasing, any unknown causes of uveitis warrant RPR/VDRL and FTA-ABS testing.
Disclosure
There are no financial or personal interests to disclose. The authors have no relevant relationships to disclose.
Disclaimer
The views expressed in this article are those of the authors and do not reflect the position or policy of the Department of Veterans Affairs or the United States government.
Consent
Written informed consent from the patient was obtained for identifiable health information included in this case report.