

Case 1: Ptosis following external radiotherapy for basal cell carcinoma
A 65-year-old white female presented for a scleral lens evaluation, referred by her cornea specialist. The patient developed right-sided radiation dermatitis and right upper lid ptosis after receiving external radiation therapy for basal cell carcinoma. The patient complained of severe ocular dryness, light sensitivity, and blurred vision.
Despite ocular surface therapies including artificial tears, topical cyclosporine, autologous serum tears, and soft bandage contact lenses, ocular symptoms persisted. The lid aperture size in the right eye was 3.0 mm and in the left eye was 10.0 mm. Marginal reflex distance 1 (MRD1) in the right eye was -1.0 mm and the marginal reflex distance 1 in the left eye was 4.5 mm. The HVID for the right eye was 11.8 mm. The right eye was fitted with a scleral lens. While significant improvement in dry eye symptoms was reported by the patient, the patient reported satisfaction and improvement in her right upper lid ptosis. The diagnostic scleral lens used was an 18.5 mm diameter lens with a spherical back surface and made using oxygen-permeable plastic, Opifrocon A (Boston Equalens II). Upon application, the diagnostic lens exhibited a fluid reservoir thickness of approximately 350 µm. The uncorrected visual acuity was 20/30 in the right eye and 20/20 with over-refraction.
Changes to the scleral diagnostic lens were made to further amplify cosmetic benefits. An 18.5 mm diameter lens with toric haptics was used to better align the back surface. The lens vault was increased by 300 µm to further increase the sagittal depth of the lens. After lens settling, there was approximately 500 µm of fluid reservoir thickness. Marginal reflex distance 1 of the right improved to 4.0 mm, with an approximate 5.0 mm improvement in ptosis severity (Figure 1). The patient was satisfied with these results.
__ptosis_in_right_eye_(b)__5.0_mm_improvement_in_ptosis_severity_with_scleral_lens_in_r.png)
The patient’s cornea was monitored following lens dispensation at one week, one month, and every six months thereafter. No clinically significant signs of corneal edema or hypoxia were noted during follow-up appointments. The patient was able to successfully continue scleral lens wear for nine years, and the improvement in ptosis stayed about the same throughout follow up visits.
Case 2: Ptosis in a patient with amyotrophic lateral sclerosis
A 43-year-old white male presented with his spouse and nurse caregiver for a scleral lens evaluation. The patient had a medical history of advanced amyotrophic lateral sclerosis and was on life support. He had difficulty opening his eyelids, secondary to progressive muscle weakening, which was exacerbated by ocular surface dryness. Because of his poor ability to open his lids, he had difficulty communicating through his Augmentative and Alternative Communication device, thereby profoundly impacting his quality of life.
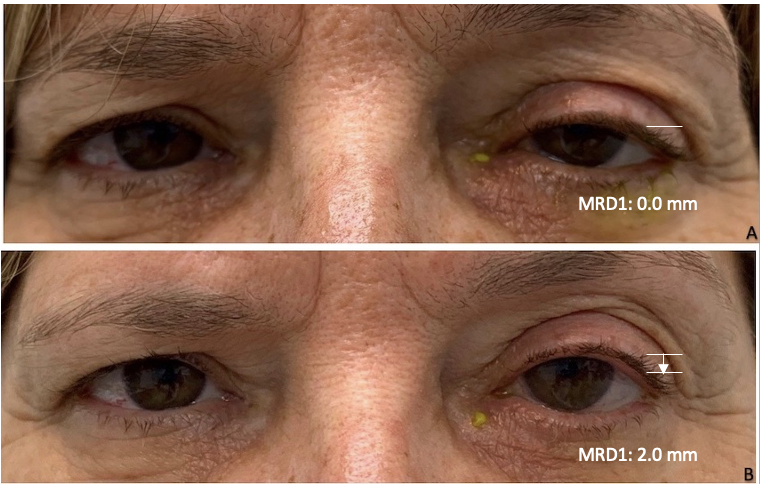
The patient’s current dry eye treatment included viscous artificial tears every hour. His symptoms were constant, and he reported ocular irritation and light sensitivity. The patient had tried the use of a ptosis crutch with his glasses, but this method proved to be uncomfortable and worsened his dry eye symptoms. Slit lamp findings revealed 3+ conjunctival hyperemia and eyelid edema. The lid aperture size in the right eye was 1.0 mm and in the left eye was 3.0 mm. Marginal reflex distance 1 in the right eye was -5.0 mm and marginal reflex distance 1 left eye was -3.0 mm. The HVID for the right & left eyes were 11.5 mm and 11.5 mm. Diagnostic scleral lenses with a diameter of 17.5 mm were trialed on the day of the consultation, and an immediate change in lid aperture was observed (Figure 2). The diagnostic scleral lenses with spherical back surfaces showed superior and inferior edge lift, as seen with a portable slit lamp.
__bilateral_ptosis_(b)__bilateral_ptosis_improved_with_scleral_lens_in_both_eyes.png)
The final scleral lenses were ordered in a 19.0 mm diameter with “With-the-Rule” toric haptics for better scleral alignment. After six hours of settling, the fluid reservoir thickness of the right and left scleral lenses were approximately 500 µm and 400 µm, respectively. Best corrected visual acuity with glasses was 20/125 in the right eye and 20/80 in the left eye. After scleral lens correction, visual acuity was 20/25 in the right eye and 20/25 in the left eye. Marginal reflex distance 1 of the right eye improved to 2.0 mm, with an approximate 7.0 mm improvement in ptosis severity. Marginal reflex distance 1 of the left eye improved to 3.0 mm, with an approximate 6.0 mm improvement in ptosis severity. The scleral lenses were made using an oxygen-permeable plastic, Hexafocon B (Boston XO2). The corneas of the patient were monitored after scleral lens dispensing at 1 week, 1 month, and 6 months. No clinically significant signs of corneal edema or hypoxia were noted at the follow-up appointments. The patient has successfully worn scleral lenses for 5 years, with stable improvement in ptosis.
Case 3: Ptosis in a patient with dry eye syndrome and recurrent corneal erosion
A 57-year-old white female presented for a scleral lens consultation and was referred by her cornea specialist. The patient underwent a bilateral laser-assisted in situ keratomileusis procedure approximately 25 years prior to presentation and had a recent history of worsening dry eye symptoms and recurrent corneal erosion in the left eye. The patient underwent superficial keratectomy in the left eye to mitigate the frequency of erosion episodes.
With the use of preservative-free artificial tears, topical steroids, topical cyclosporine, and autologous serum tears, the patient still experienced severe ocular discomfort, constant foreign body sensation, redness, tearing, blurred vision and light sensitivity in the left eye. She became dependent on a soft bandage contact lens to alleviate her dry eye symptoms. In addition, the patient complained of a left upper lid drooping. The lid aperture sizes in the right eye were 8.0 mm and in the left eye was 6.0 mm. Marginal light reflex 1 in the right eye was 2.0 mm and marginal light reflex 1 in the left eye was 0.0 mm. The HVID for the left eye was 12.0 mm. The patient underwent oculoplastic evaluation for ptosis repair surgery but was decided against surgical intervention because of the risk of aggravation of dry eye symptoms. A 17.0 mm-diameter diagnostic scleral lens was placed on the left eye in the office. She reported some edge awareness with the spherical back surface trial scleral lens but noted an improvement in lid ptosis, an improvement in vision and some relief from her dry eye symptoms.
Her final scleral lens was an 18.0 mm diameter, quadrant-specific scleral lens that settled to a fluid reservoir thickness of approximately 400 µm centrally after 5 h of wear time. Her uncorrected visual acuity in her left eye fluctuated between 20/30 and 20/20. Visual acuity with the final scleral lens was 20/15. The marginal light reflex 1 of the left improved to 2.0 mm, with an approximate 2.0 mm improvement in ptosis severity (Figure 3). The scleral lens was ordered using an oxygen-permeable plastic, Opifrocon A (Boston Equalens II). The patient’s cornea was monitored following lens dispense at one week, one month, and two months. No clinically significant signs of corneal edema or hypoxia were noted during follow-up appointments. The patient has been successfully wearing scleral lenses for five years. This patient’s improvement in ptosis has been relatively stable throughout her follow up visits.
__ptosis_in_left_eye_(b)__ptosis_improved_with_scleral_lens_in_left_eye.png)
Discussion
Depending on the etiology and severity, ptosis can be managed with various surgical interventions, including levator aponeurosis advancement, frontalis sling procedure, and levator resection.2 Mild lid ptosis can be treated with a recent FDA approved topical medication, oxymetazoline hydrochloride ophthalmic solution (0.1%), an alpha adrenoceptor agonist that targets receptors on Mueller’s muscle. It is important to note that oxymetazoline hydrochloride ophthalmic solution (0.1%) mainly targets Müller’s muscle, therefore, its effects are limited in cases of lid ptosis where Müller’s muscle is not the main causative factor.
This case report series shows that scleral lenses can be used effectively to improve eyelid ptosis in patients with concurrent ocular surface disease. Whether the lenses were fit specifically for ptosis improvement, or had a secondary effect, we observed a significant improvement in ptosis in all three cases.
Scleral lenses are rarely used to manage ocular ptosis. A previous study at Moorfields Eye Hospital in London analyzed the use of scleral lenses in 1,560 eyes. Of the 1,560 eyes fit in scleral lenses, only 14 eyes were fit for the purpose of ptosis improvement.3 A retrospective case review and several case reports have illustrated the use of scleral lenses for ptosis improvement.2,4,5
It is theorized that the main contributing factor to ptosis improvement is increased bulk of the scleral lens, resulting in a shelf for the upper eyelid to sit. In the past, a method using scleral lenses for ptosis incorporated a ptosis prop or ledge on the surface of the lens.6 This type of design had various complications including the inability to blink and patient discomfort. Instead, adjusting several parameters to increase the sagittal height of the lens has been shown to be helpful.
Larger diameter lenses allow for an increased sagittal depth with a broader weight distribution on the sclera. This size is also the lens of choice in patients with ocular surface disease to aid in support of the cornea and adjacent conjunctiva. All patients in this case series were fitted in lenses with a diameter of 6 mm or greater than HVID to be considered a large scleral lens. In addition to increasing lens diameter, sagittal depth can be increased by altering base curve and secondary curves. These changes increase the fluid reservoir thickness of the lens. The average recommended fluid reservoir thickness in a standard fit is 100–200 µm. When fitting patients specifically for ptosis improvement, an intentionally excessive fluid reservoir thickness of 400–600 µm is clinically used. Of note, there are studies in which increased central fluid reservoir thickness were used to improve lid ptosis,2,4,5 and there were no reports of corneal compromise, such as corneal edema or corneal neovascularization, like that in our three cases.
It is important to highlight the possible complications of fitting scleral lenses with excessive fluid reservoir thickness. One of the first in vitro studies examining scleral lens wear and hypoxia revealed that oxygen delivery to the cornea is reduced by 30% for a 400-micron tear reservoir compared to the recommended 200 microns.7 This study, along with theoretical models, suggests reducing lens thickness and reservoir thickness for the reduction of potential hypoxic stress. Another study showed that lens-induced central corneal edema increases with increasing reservoir thickness, but plateaus at a thickness of around 600 μm.8 In addition to potential corneal edema, excessive clearance can lead to other complications including reservoir debris, blurry vision, lens decentration and lens discomfort. The patients in this case series did not experience any of these complications.
To reduce potential hypoxic stress in an eye fitted with an excessive reservoir thickness, it is prudent to fit these patients in hyper or ultra-Dk material. Tisilfocon A (Dk 180) and Fluoroxyfocon A (Dk 200) may be a good choice for fitting highly vaulted scleral lenses. During the time of fitting of our patients, these materials were not FDA approved. Ancillary testing including specular microscopy and pachymetry may be useful in fitting scleral lenses for ptosis. Patients fitted with excessive reservoir thickness need to be closely monitored for any signs of corneal hypoxia, including clinically significant corneal edema or neovascularization. Ultimately, fitting a scleral lens to improve ptosis requires a risk vs. benefit analysis that must be discussed with the patient and other members of the co-management team.
It is important to acknowledge that this is an anecdotal report of three patients that cannot be considered proof of the effectiveness of scleral lenses to improve ptosis. Research in the form of controlled, randomized studies would be required to validate the approach to ptosis improvement. Further studies could explore how varying reservoir clearances and lens diameters affect ptosis improvement.
Conclusion
This case series highlights the use of scleral lenses for ptosis management in patients with concurrent ocular surface disease. It suggests a non-surgical or non-pharmacological alternative for ptosis improvement leading to improved cosmesis and, in some cases, vision. The use of scleral lenses offers an alternative method for improving ptosis but does not go without potential complications.
Disclosures
The authors have no financial or proprietary interest in any material or method mentioned in this article. This article has been peer reviewed.