
Introduction
The most common form of uveitis is anterior, and the most common identifiable causes are HLA-B27-associated conditions e.g. ankylosing spondylitis, inflammatory bowel disease, psoriatic arthritis and reactive arthritis, Fuchs heterochromic iridocyclitis and herpetic uveitis.1 Lyme Borreliosis (LB) accounts for less than 1% of all uveitis cases. Appropriate clinical suspicion for systemic LB as well as incomplete resolution on systemic corticosteroid monotherapy are necessary to make a diagnosis of Lyme-associated uveitis (LAU). Those criteria were essential in distinguishing the cause of the uveitis in a case of post-fever retinitis (PFR) in a LB seropositive patient described herein.
Case Presentation
A 66-year-old male presented to the eye clinic for a problem visit with chief complaint of blur and foreign body sensation that began four days prior after getting sawdust in his right eye. The patient had a history of right orbital floor fracture without extraocular muscle entrapment five years prior to presentation. He was also a glaucoma suspect secondary to large cupping in both eyes.
The patient’s medical history was remarkable for hypertension, hyperlipidemia, and psoriatic arthritis for which he was prescribed methotrexate 12.5mg per week. He also had previous history of symptomatic LB about ten years prior to presentation for which he was treated. His most recent enzyme immunoassay (EIA) and Western Blot were three years prior to presentation and were both positive at the time. He had no recent history of tick bite or erythema migrans rash.
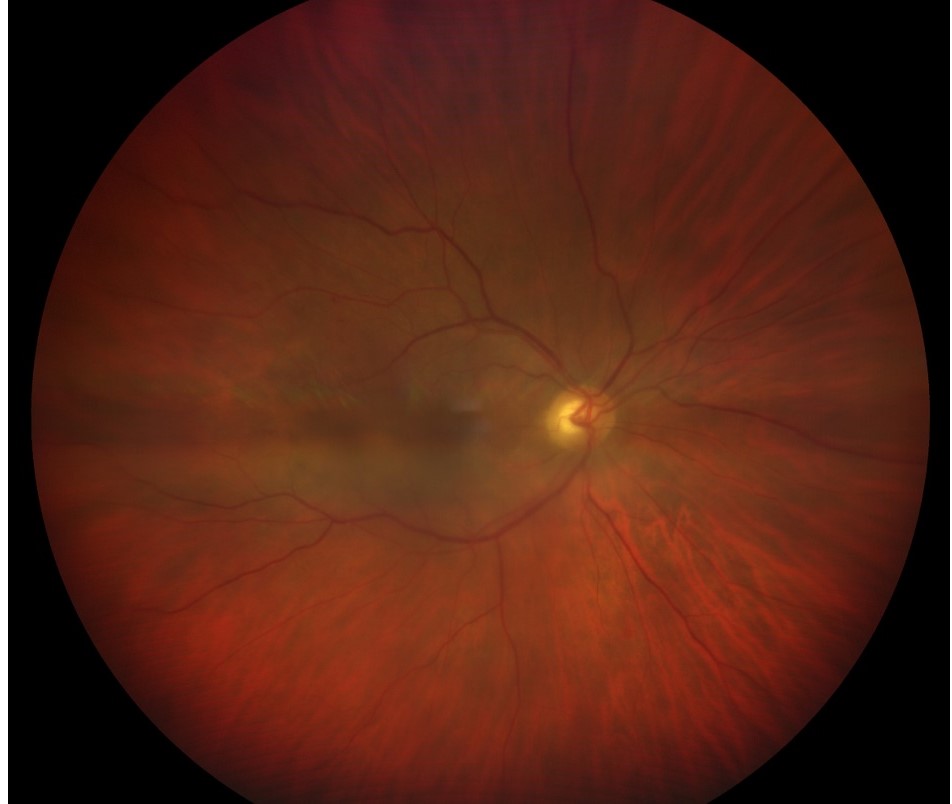
His entering visual acuity (VA) was 20/100 without improvement on pinhole in his right eye, and 20/25+2 in the left eye. Pupils, extraocular motility, and confrontation fields were all unremarkable. There was 1-2+ anterior chamber cells and anterior vitreous cells in his right eye. The left eye showed no cells or flare. His intraocular pressure (IOP) measured 18mmHg in his right eye and 21mmHg in his left eye at 8:20 am. On dilated fundus examination, there was 1+ nuclear sclerosis OU and 1+ vitreous cell and haze in the right eye with resulting hazy view of the retina (Figure 1). The vitreous was clear and acellular in the left eye. There were scattered intraretinal hemorrhages in the posterior pole of his right eye. There was no retinal hemorrhage noted in the left eye. There was no snowbanking, snowballs or granulomata in either eye.

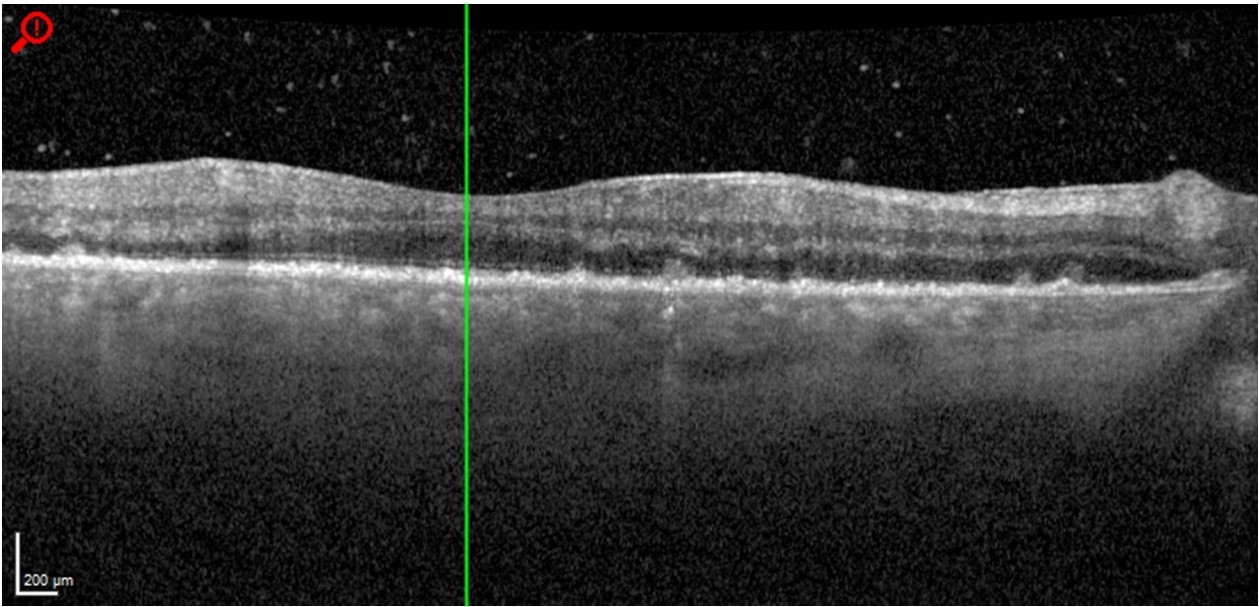
Macula optical coherence tomography (OCT) of the right eye showed hazy media due to the vitritis with visible vitreous cells in the posterior vitreous (Figure 2). The foveal contour was normal and there was no intraretinal or subretinal fluid. The retinal pigment epithelium (RPE) showed marked irregularity with numerous small hyperreflective nodules at the level of Bruch’s membrane consistent with inflammatory deposits and 2 small pigment epithelial detachments (PED), approximately 100µm each in size just temporal to the optic nerve. Macula OCT of the left eye was unremarkable.

Management and Outcomes
The patient was diagnosed with panuveitis of the right eye and was prescribed topical ophthalmic prednisolone acetate 1.0% one drop in the right eye every two hours while awake. The patient was to return to clinic in three days to monitor for changes and referred to the next available uveitis clinic in one week. Serology was ordered including CBC, Lyme EIA and Western Blot, serum ACE, RPR, FTA-ABS, T-Spot, ESR, CRP, and ANCA. Exam findings were stable at three day follow up with a mild reduction in anterior chamber cell/flare noted.
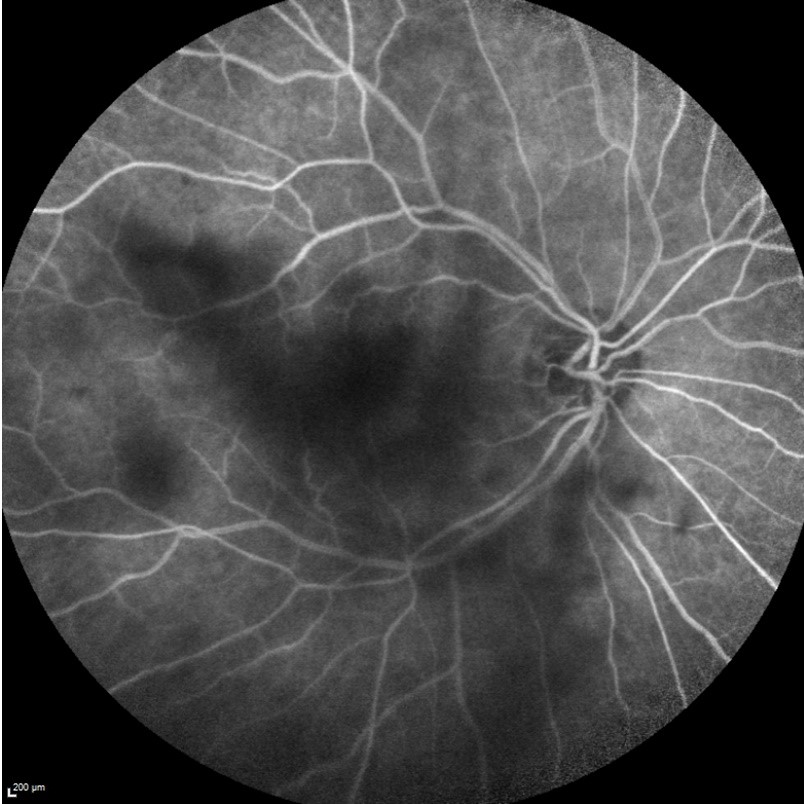
At the follow up examination in the uveitis clinic, the patient’s VA had improved to 20/70 in the right eye, and the exam was otherwise stable. Fluorescein angiography of the right eye showed a blocking defect due to vitreous opacity; there was no leakage/staining of the disc or retinal vasculature (Figure 3). Serology revealed positive LB IgG and IgM on EIA and Western Blot. All other testing was unremarkable. Further history revealed that the patient experienced two episodes of acute fever as high as 103℉ about two weeks apart approximately two months prior to his initial presentation. Given the absence of any systemic symptoms of LB, this aspect of his presentation was considered integral in elucidating the cause of his intraocular inflammation. The patient was diagnosed with PFR. Prednisolone acetate was discontinued, and the patient was prescribed oral prednisone 40mg per day and was to return to clinic in eight days.

Over seven weeks, the anterior and vitreal inflammation and RPE disruption improved until the eye was quiet and macula OCT appeared normal (Figure 4). At this point, VA had improved to 20/40 in the right eye. The patient was eventually tapered off prednisone over a period of nine weeks. Near the end of the taper, there were IOP spikes secondary to the steroid reaching 34mmHg OD and 30mmHg OS . The patient was prescribed dorzolamide/timolol ophthalmic solution to lower IOP until the steroid taper was completed. Eight weeks later the eye remained quiet with stable IOP and VA recovering to 20/25 OU.

Discussion
This case illustrates challenges of a case of diagnosing an alternative cause of uveitis in a patient with known history of LB and positive serologies. The clinical history, exam findings, and response to treatment were more suggestive of PFR than LB-associated panuveitis.
Post-Fever Retinitis
Post-fever retinitis is ocular inflammation that can occur following febrile illness.2,3 This typically manifests with various retinal findings, and the cause of the illness is most often due to viral, bacterial, or protozoal etiology.2,4 Most documented cases have been in tropical countries.3,4
The onset of ocular symptoms typically begins 2-4 weeks after the fever in immunocompetent individuals but can take up to two months to manifest.2–4 Due to this delayed onset, it is often difficult to isolate the exact causative etiology of the illness, and systemic symptoms are often fading or resolved by the time the patient seeks care with an optometrist or ophthalmologist.2,4 Thus, patients who do not seek care for the initial fever are less likely to have an identifiable etiology. In studies where post-fever uveitis diagnosis did not exclude unknown causative etiology, idiopathic cases composed the majority of cases.3 The delayed presentation suggests that there is an immunological basis for the condition.2
The most common symptom is sudden, painless diminution of vision.2 Ocular findings are consistent irrespective of the cause of initial illness.2 Post-fever retinitis can present unilaterally or bilaterally.2 Some studies report equal incidence between the two, while others report a greater preponderance for bilateral presentation.2,3 Ocular findings are similar regardless of laterality.2 Posterior segment findings include focal or multifocal retinitis at the posterior pole, most often in the peripapillary area.2 Macular edema is present in approximately half of the cases (55.12%).3 Most patients will have vitritis, and at least 1 study noted vitritis in 100% of cases (n=14).2,3 A mild to moderate anterior chamber reaction has also been reported in 18.05% of cases in one study.3
In most cases, PFR is self-limiting, and some physicians prefer observation over medical therapy.4 When medical therapy is used, corticosteroid therapy is most commonly used for PFR, though antibiotic or anti-viral therapy have been reported.2–4 Most cases resolve over 2-4 months with VA improvement regardless of causative etiology.2,3
Lyme-Associated Uveitis
Lyme Borreliosis is rare, even in endemic regions, accounting for less than 1% of all uveitis cases, and serology should not be ordered without appropriate clinical suspicion.5 A recent history of tick bite accompanied by an erythema migrans lesion, recent-onset arthritis or a facial nerve palsy warrant serological screening for LB.5–8 Clinical characteristics of LAU are variable, and it can present in all anatomic forms of uveitis.5 There is no established gold standard or criteria for diagnosis of LAU and positive serological screening alone is insufficient to confirm that a patient has LB.5,6,9
There are common criteria shared within the literature on LAU, however. There must be a clinical probability based on possible exposure and absence of other causative etiologies.5,6,9 In addition, an incomplete response to corticosteroid monotherapy is used as a criterion.5,6 Cases defined as LAU all resolved with the addition of antibiotic therapy, and when used together, antibiotics and corticosteroids are effective in reducing inflammation and improving vision.5–7,9
The challenge in diagnosing LAU is differentiating whether positive Lyme serology status is incidental or causally connected.6 Serum IgM and IgG can remain positive for years post-treatment.5,6 Therefore, regular screening for LB antibodies in uveitis patients is of limited value even in endemic regions and can lead to frequent false positives.5,6,9 However, selective screening can be beneficial in cases of unknown origin, particularly in patients with vitritis, incomplete response to corticosteroid therapy, or systemic symptoms of LB.9
Conclusion
In the absence of suspicion for LB and with unremarkable lab workup, it is useful to inquire about a recent history of febrile illness preceding the onset of symptoms. The delayed onset of ocular symptomatology in PFR poses a challenge, as it is difficult to diagnose a causative etiology weeks after resolution of fever even when utilizing exhaustive serology. Cases of PFR will often resolve after initiation of systemic corticosteroid monotherapy.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Funding
The authors have no financial or proprietary interest in any material or method mentioned in this article. This article has been peer reviewed.