

Case Report
A 63-year-old African American male presented with a complaint of a ptotic superior left lid. The ptosis was constant and did not vary through the day or with fatigue. He first noticed the ptosis two weeks earlier after being discharged from the hospital for treatment of COVID-19 related pneumonia which required him to be on a ventilator the previous two and a half months. He was prescribed 60 mg of oral prednisone upon discharge for the treatment of persistent pulmonary symptoms and instructed to follow-up with his primary care physician for tapering. His other major medical diagnoses included type 2 diabetes mellitus, hypertension, dyslipidemia, sleep apnea, and gout.
Best-corrected visual acuity measured 20/20 in each eye. Extraocular muscle function and confrontation visual field testing was normal in both eyes. Anisocoria was noted with the right pupil measuring 7 mm and the left measuring 4 mm in dim lighting. In bright lighting, the right pupil measured 5 mm and the left measured 2 mm. Each pupil reaction was brisk and no afferent pupillary defect was present OU. Ptosis of the superior left lid was apparent with unequal palpebral fissure heights measuring 10 mm on the right and 6 mm on the left. Anterior segment findings were unremarkable in each eye. Intraocular pressures measured 13 mmHg OU at 9:14 am, and dilated fundus examination revealed healthy optic nerves, maculae and peripheral retinae.
Based on the presence of left upper lid ptosis and pupil miosis, (Figure 1), diagnostic testing for suspected Horner’s syndrome was initiated. One drop of 0.5% apraclonidine was instilled in each eye and the patient was evaluated thirty minutes later to monitor for changes in pupil size and palpebral fissure height. Upon re-evaluation, the ptosis of the left upper lid was almost completely resolved and the previously miotic left pupil was dilated (Figure 2), confirming our suspicion of Horner’s syndrome.


The case was reviewed with neurology and the following tests were ordered: MRI/MRA of the head and neck with and without contrast, CT of the chest, carotid ultrasound, CBC, and erythrocyte sedimentation rate. No significant abnormalities were noted on MRI/MRA, carotid ultrasound, or blood work. However, CT images of the chest revealed upper lobe atelectasis, which is a complete or partial collapse of an area of the lung, as well as pleural effusion or abnormal fluid collection in the pleural cavity. After evaluation by neurology and a thorough review of the patient history and ancillary testing, it was determined that the Horner’s syndrome was due to cervical and upper chest trauma, as well as inflammation secondary to prolonged intubation.
When the patient was discharged from the hospital follow-up care was coordinated with his primary care provider who slowly tapered the oral steroids over the following one-month period. At his six-month follow-up visit with the eye clinic he was noted to have minimal residual ptosis and only 1 mm of persistent anisocoria. Improvement of the ptosis and miosis was attributed to the resolution of inflammation. These findings have remained unchanged over the last twelve months and will likely persist due to trauma to the cervical and chest wall that occurred during intubation.
Discussion
Horner’s syndrome is the name given to the clinical presentation of oculo-sympathetic paresis.1 It was named for the Swiss ophthalmologist, Johann Friedrich Horner, who published a case report on the condition in 1869. It is also referred to as Claude Bernard-Horner syndrome as Claude Bernard first recognized the triad of symptoms associated with the disease in 1852 using animal models.2 Horner’s syndrome occurs in approximately 1 per 6,000 people worldwide making it an uncommon condition. Horner’s syndrome affects males and females equally, and it may occur at any age affecting both pediatric and elderly populations. There is no predilection for Horner’s syndrome in any geographic location or in any ethnic group.3
Horner’s syndrome is characterized by the classic triad of ptosis, miosis, and anhidrosis. Ptosis associated with Horner’s syndrome occurs due to a lack of sympathetic tone within Muller’s muscle of the upper eyelid, which leads to narrowing of the palpebral fissure on the affected side.4,5 Miosis occurs on the affected side due to a decrease in sympathetic tone to the iris dilator muscle, which leaves the parasympathetic tone of the iris sphincter muscle unopposed. Delayed dilation or “dilation lag” moving from bright to darkened lighting conditions may also occur due to the lack of contribution by the sympathetic system to the iris dilator muscle. Ipsilateral facial anhidrosis occurs due to interruption of the sudomotor system that is responsible for perspiration.6
Causative lesions of Horner’s syndrome are divided into first, second, or third order lesions (Table 1), also referred to as central, preganglionic, or postganglionic. First order (i.e. central) neuron cell bodies are located in the hypothalamus and their axons descend through the brainstem and spinal cord to reach the ciliospinal center of Budge-Waller at level C8 to T2.6 First order lesions of these neurons often show different symptoms depending on the type of lesion. Lesions of the hypothalamus and thalamus, such as infarct, tumor, or hemorrhage, present with an ipsilateral Horner’s syndrome that can be accompanied by contralateral hemiparesis and hypesthesia. Dorsal midbrain lesions are a type of first order lesion that can result in an ipsilateral Horner’s syndrome accompanied by a 4th cranial nerve palsy.7 Horner’s syndrome resulting from lesions of the pons can also have ipsilateral or bilateral abducens palsy. Some other types of first order lesions include Wallenberg syndrome and cervical or upper thoracic spinal cord lesions.6
Second order (i.e. preganglionic) sympathetic neurons exit the ciliospinal center of Budge-Waller forming a sympathetic nerve that passes under the aorta and over the apex of the lung. The neurons then pass through the stellate ganglion, up the carotid sheath, and synapse at the superior cervical ganglion at the level of the carotid bifurcation.11 Lesions of the upper chest such as Pancoast tumor, trauma to brachial plexus or soft tissue of the neck, and pneumothorax can result in Horner’s syndrome.8
Third order (i.e. postganglionic) neurons originate in the superior cervical ganglion, travel up the common carotid artery, and then continue to travel along the internal carotid as a plexus. A more defined nerve is then formed within the cavernous sinus that travels along the 6th cranial nerve, joins the ophthalmic division of the trigeminal nerve, and enters the orbit to reach the eye via the superior orbital fissure.11 Lesions of the neck, skull base, and orbit can cause a third order neuron Horner’s syndrome. Some examples of conditions that may cause a third order neuron Horner’s syndrome include carotid dissection, cluster headaches, cavernous sinus lesions, and rare tumors of the skull base. Carotid dissection is the most common causative lesion of third order neuron Horner’s syndrome accounting for 20-30% of patients diagnosed with Horner’s syndrome6
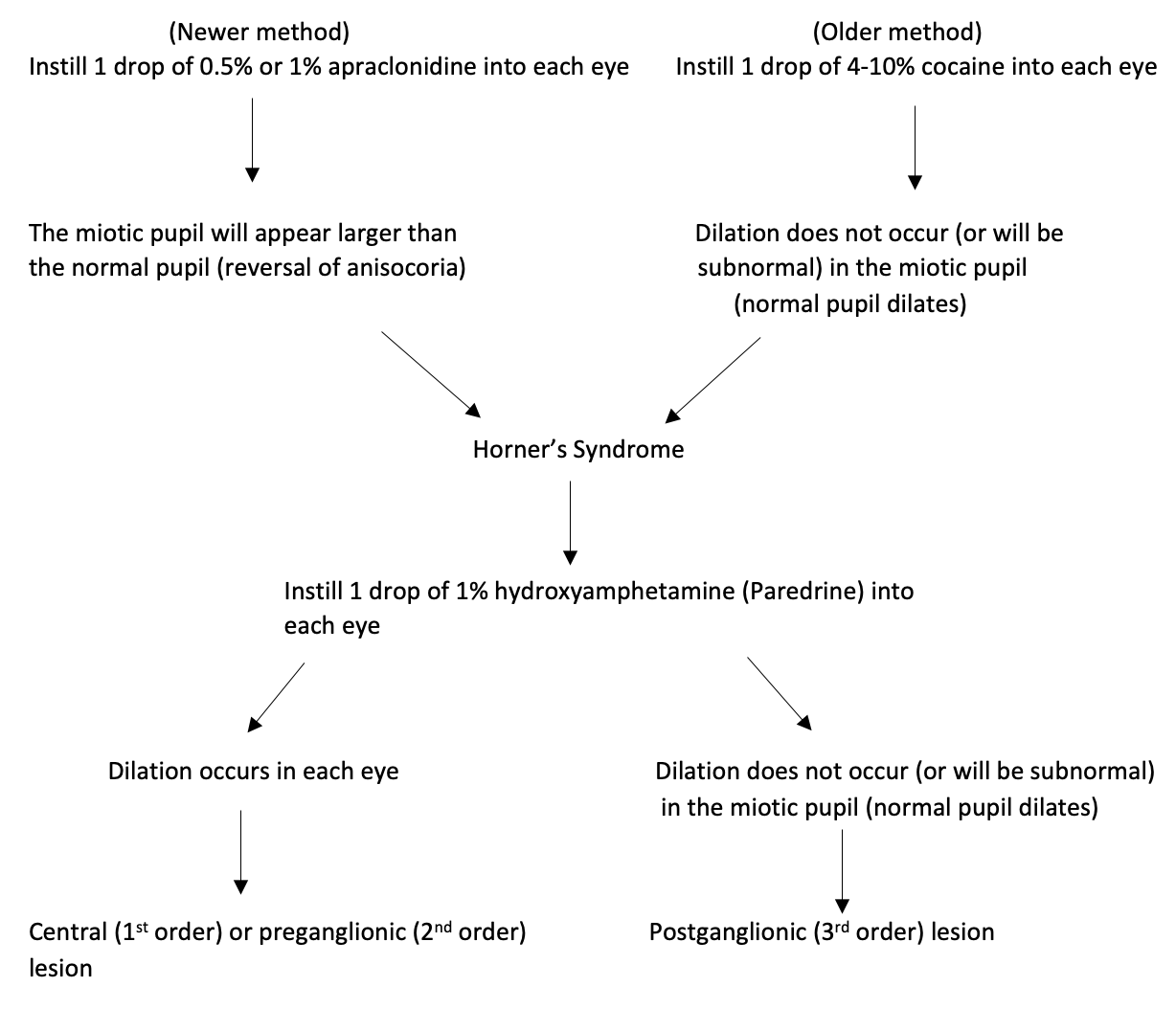
Confirmation of suspected Horner’s syndrome can be achieved with ophthalmic pharmacological testing (Table 2). The preferred agent for pharmacological testing is 0.5% apraclonidine ophthalmic solution. One drop is instilled in each eye and the examiner waits 30 minutes before determining the response. Horner’s syndrome is confirmed if the anisocoria reverses (i.e. the smaller pupil will become larger in size than the fellow eye). The dilation of a Horner’s pupil occurs using a weak sympathetic alpha-1 agonist such as 0.5% apraclonidine due to denervation super-sensitivity of the alpha-1 receptors on the iris dilator muscle.12 Apraclonidine 0.5% will also reverse the ptosis of Muller’s muscle associated with Horner’s syndrome due denervation super-sensitivity of the alpha-1 receptors of the smooth muscle.5

The alternative, historical method of pharmacological testing for Horner’s syndrome was the use of topical 4-10% cocaine eyedrops. Cocaine blocks the reuptake of norepinephrine by the presynaptic membrane leaving a greater quantity of norepinephrine remaining in the synaptic cleft. This leads to pupil dilation in normal patients. In a patient with Horner’s syndrome, the normal pupil will dilate, but the Horner’s pupil remains unchanged (miotic) due to the lack of a baseline amount of norepinephrine present in the synaptic cleft.12 Topical cocaine is no longer used due to several disadvantages including a short shelf-life, status as a controlled substance, and limited availability.
Localization of the lesion in patients with Horner’s syndrome can be achieved using topical 1% hydroxyamphetamine ophthalmic solution (Paredrine). Hydroxyamphetamine will dilate a normal pupil and a Horner’s pupil if the third order neuron is intact since hydroxyamphetamine causes direct release of norepinephrine from intact presynaptic nerve endings. Therefore, if the affected pupil of a Horner’s syndrome patient dilates with 1% hydroxyamphetamine, the lesion must be at the level of either a first or second order neuron. If the affected pupil does not dilate with hydroxyamphetamine, the cause of the Horner’s syndrome must be a postganglionic or third order lesion.6
Identifying the exact cause of a Horner’s syndrome may entail extensive testing due to the large anatomic area encompassed by the sympathetic pathway (Table 3). Evaluation may be tailored to some extent if the patient presents with additional symptoms which point more specifically to a causative lesion. However, most patients present with isolated Horner’s syndrome and therefore require imaging along the complete oculosympathetic pathway. This includes MRI/MRA or CTA of the head and neck extending down to the aortic arch, and CT of the chest.6,11
The novel SARS-CoV-2 (COVID-19) is a form of coronavirus that can result in potentially fatal respiratory failure. SARS-CoV-2 was declared by the World Health Organization (WHO) to have reached pandemic status in March of 2020.13 Hospitalization with eventual intubation and mechanical ventilation was not uncommon during the height of the COVID-19 pandemic due to its variable and severe respiratory complications. As trauma and inflammation may result from the process and/or duration of intubation, this requires consideration as a potential etiology of Horner’s Syndrome, as was the case with our patient.
The literature currently available regarding the ocular manifestations and ocular sequelae of COVID-19 is limited, but the most commonly reported ocular association is conjunctivitis along with a few reports of retinal vascular occlusion.14 This case demonstrates an additional potential ocular complication that may arise related to the COVID-19 virus and its subsequent treatment.
Conclusion
Horner’s syndrome is a relatively uncommon condition with many possible causative lesions. Once the diagnosis of Horner’s syndrome is confirmed with ophthalmic pharmacological testing, it is important to uncover the underlying cause in a timely manner, as certain etiologies of Horner’s syndrome can prove fatal if untreated. This case outlines the novel presentation of transitory Horner’s syndrome secondary to cervical and upper chest trauma associated with prolonged intubation for the treatment of respiratory complications from COVID-19 infection. This review emphasizes the necessity of a thorough case history, appropriate testing, and interdisciplinary collaboration.
Funding
The authors have no financial or proprietary interest in any material or method mentioned in this article. This article has been peer reviewed.