INTRODUCTION
Laser pointer retinopathy occurs when there is injury to retinal tissues from handheld laser devices that are accidentally or intentionally directed at the eye. Patients can often present with no symptoms at all or can complain of blurry vision, scotomas, and metamorphopsia.1–4 The most common posterior segment findings in these individuals are unilateral or bilateral pigment changes alongside circumscribed, yellow chorioretinal scars located at the fovea.5–7 Optical coherence tomography (OCT) imaging is indicated to aid in diagnosis as focal retinal pigment epithelium (RPE) loss and foveal ellipsoid zone disruption are characteristic findings.3,8–10 Treatment is limited since there are no effective evidence-based medical treatments and self-resolution is common.2 Therefore, these patients are managed with regular follow-ups to monitor for changes or potential trauma-related sequelae and education to avoid laser pointer exposure.
CASE REPORT
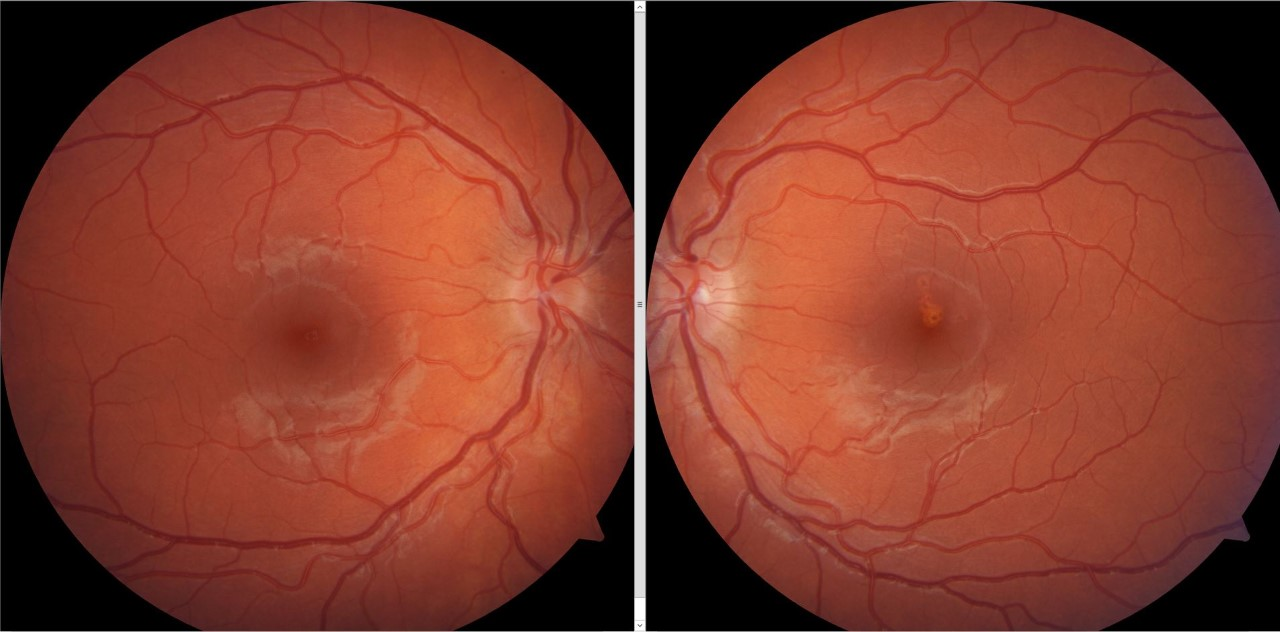
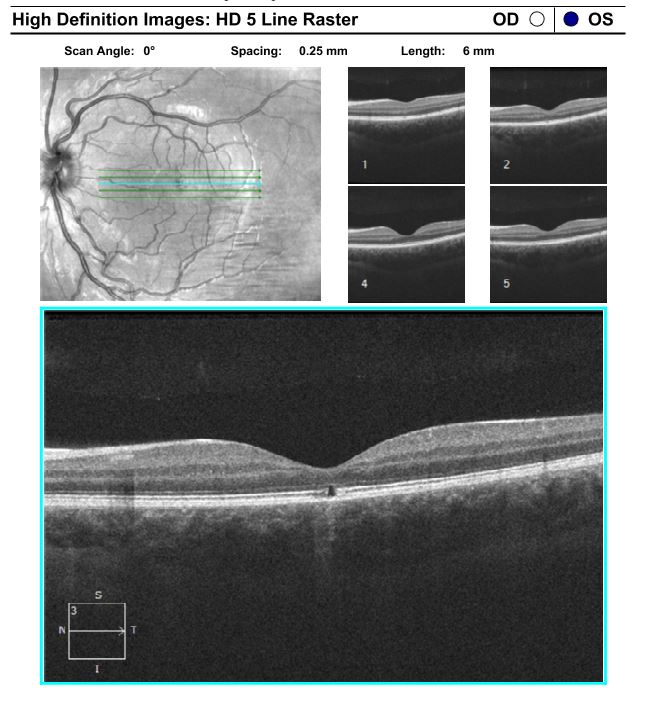
A 19-year-old male reported to the eye clinic for a routine eye examination. He complained of slight distortion inferior to central fixation in the left eye. He denied any distortion or scotoma in the right eye. Upon further questioning, the patient admitted that his symptoms had been longstanding and stable for the past few years, and only noticeable when looking through the left eye. Ocular and medical history were unremarkable for him and his family. Upon examination, the patient’s best corrected visual acuity was 20/15 in both the right and left eye. Pupils were both equal, round, and reactive to light with no afferent pupillary defect. Confrontation visual fields and extraocular motility testing were full in both eyes. Slit lamp biomicroscopy findings and intraocular pressures were within normal limits. Intra-ocular pressures with Goldmann tonometry were noted at 14mmHg in each eye. Dilated fundus examination of the right eye showed a flat and clear macula with a normal retinal periphery that was free of any breaks or detachments. The optic nerve was flat and distinct with a cup to disc ratio of 0.2/0.2. Dilated fundus examination of the left eye revealed a coalesced yellow area of scarring/atrophy in the macula that slightly extended superior to the fovea (Figure 1). Optical coherence tomography was performed with the results being unremarkable in the right eye. However, the OCT in the left eye demonstrated a central cavitation defect at the level of the ellipsoid zone (Figure 2). These findings corresponded with Amsler grid testing which confirmed slight distortion inferior to central fixation in the left eye while being unremarkable in the right eye. Differentials at this time included laser pointer maculopathy, solar retinopathy, eclipse retinopathy, and partial thickness macular hole. The patient was questioned about sun and eclipse gazing and denied both. He did confirm however that he did have an extended period of time playing and viewing with laser pointers a few years prior and that it coincided with the onset of the visual distortion.


Based on the case history and presentation of findings on the fundoscopic examination along with OCT findings, the patient was diagnosed with laser pointer retinopathy in the left eye. Management was conservative due to the location of the intrafoveal photoreceptor loss and stability of findings. The patient was advised to follow-up annually to monitor the condition and heavily educated on the importance of avoiding lasers, especially near the eye.
DISCUSSION
Lasers have been utilized in professional settings for years, ranging from handheld classroom devices to various health care and military devices. Recently, however, they have become much more accessible to the public and to individuals that have not received proper safety and handling education. They are often included in children’s toys and sold online with improper labelling or poor regulation. As a result, laser pointer ocular injuries have been increasingly more prevalent in pediatric and adolescent populations.2,6,11
In the United States, the Food and Drug Administration’s (FDA) Center for Devices and Radiological Health (CDRH) regulates the manufacture of lasers and their use in medical, surveying/alignment and demonstration settings.3 They provide classifications for lasers based on their output power and are outlined as class I, class IIa, class II, class IIIa, class IIIb and class IV. According to the FDA, lasers can only be sold as “laser pointers” if they are less than 5 mW (class IIIa). However, “handheld lasers” can be more powerful and range from 5 mW to 500 mW (class IIIb) or greater than 500 mW (class IV).12 These lasers pose ocular hazards as class IIIa lasers are dangerous if the beam is even briefly viewed directly, and classes IIIb and IV can cause immediate skin and eye hazard if viewed directly.13 While the FDA monitors the safety profiles of lasers in professional settings, handheld lasers that are used recreationally are not as well regulated.2 As a result, these lasers are readily available for purchase online and are often improperly labeled as belonging to a lower class compared to their true power outputs which poses a grave ocular hazard.6
The mechanism through which lasers typically cause injury to retinal tissue is via thermal damage and photochemical toxicity.1,14 The photochemical energy emitted by the laser pointer cannot be absorbed by the RPE, which causes localized tissues to heat with resultant tissue oxidation, free radical formation and photoreceptor cell death.2,9 The amount of damage to retinal tissue depends on the laser’s wavelength, laser distance to eye, radiation power, period of exposure, and spot size.13 Case series have revealed that even a single exposure of laser) output (accidental or intentional), with durations anywhere between 3 to 10 seconds, was enough to cause symptoms in younger children and teenagers.6,15 Additionally, this damage is more prominent with green laser pointers since they contain a shorter wavelength of light (wavelength 490-575 nm), which the retina is more sensitized to, compared to red laser pointers that contain a longer wavelength of light (wavelength 635-750 nm).2,10
Children are at an increased risk of laser eye injury due to their greater interest in laser appearances and lack of awareness of the damage they can cause.8 Misuse has been associated not only with accidental exposure but also intentional exposure including “games” in which children would try to determine who could withstand laser exposure into the eye for the longest period of time.16 Additionally, children have a clearer ocular media and are less likely to employ the same protective mechanisms of blinking and gaze aversion in response to lasers directed at the eyes when compared to adults.13 It has often been reported that children with behavioral problems and learning and mental health issues are at a higher risk of ocular injury since they are more likely to partake in self-injurious behavior.13 Thus those with attention deficit hyperactivity disorder and autism are commonly associated with intentional injuries.13 Individuals with these conditions and laser pointer injuries may not present with a clear case history which can lead to a delayed diagnosis as other differentials may be unnecessarily considered.
Differentials include conditions that are classified under the umbrella term photic retinopathy, conditions that are secondary to damage from light of variable sources and wavelengths.1 This includes laser pointer retinopathy, solar/eclipse retinopathy, and arc welding retinopathy.
Solar maculopathy/eclipse maculopathy: Solar maculopathy and eclipse maculopathy are both conditions that are a direct consequence of viewing the sun with retinal damage resulting in as little as one to a few minutes of extending viewing.1,17,18 This results in a retinal appearance and signs and symptoms that are like laser pointer maculopathy. The condition usually occurs more so during extended viewing of solar eclipses. However, it can also occur secondary to periods of psychoses, religious ceremonies, and outdoor sporting events.19 Although one should remember viewing the sun for a period of time, many patients cannot recall viewing the sun. One retrospective study noted that 49% of patients that were diagnosed with solar retinopathy could not remember if they had ever stared at the sun.20 Our patient had no known history of any sun gazing.
Arc welding is a rarer form of photic retinopathy that is a direct result of viewing lasers used to bind metals without proper laser filtering eye protection. The pathophysiology and signs and symptoms are again similar to those seen with the other photic retinopathy conditions.21 Our patient again denied any history of welding or exposure to lasers used in welding. Physicians should also note if one or both eyes are involved. Solar and arc retinopathy are more likely to present bilaterally when compared to laser retinopathy which can bilateral but is more likely to present unilaterally.1
In cases where children do not present immediately following the laser pointer injury, they can sometimes be misdiagnosed with a macular dystrophy due to their retinal appearance.7 In the presence of these findings, more pointed case history questioning is warranted to determine the causative agent. Furthermore, the stability of the retinal findings is meaningful in differentiating this condition from other hereditary macular dystrophies which are slowly progressive and occur bilaterally.4 Family history and genetic testing are also paramount, as a hereditary dystrophy may be present in one or more family members when compared to laser pointer maculopathy.
OCT imaging is key in diagnosing laser pointer retinopathy. Characteristic findings can include interruption and damage to the ellipsoid zone with subsequent retinal pigment epithelium loss.13 Hyper reflective bands in a vertical orientation can also be seen at the level of the outer retina.4 Other diagnostic imaging can further aid in the diagnosis. This includes multimodal testing such as such as OCT-angiography (OCT-A) and fluorescein angiography. There will be corresponding areas of choriocapillaris closure on OCT-angiography and delayed foveal hyper fluorescence along with RPE window defects on fluorescein angiography.9,13 Furthermore, OCT-A has shown that in addition to the RPE being damaged, the laser may penetrate to the choriocapillaris and can present as hypointense lesions or low signal areas.14,22 Fundus autofluorescence, however, does not provide as much value since it will reveal varied areas of normal, hypo- and hyper-autofluorescence which does not provide a clear clinical picture.7
While some patients may be asymptomatic or mildly symptomatic and have this condition incidentally uncovered during a routine exam like our patient, other patients will present immediately following the laser pointer accident with varying symptomatology. These symptoms include reduced vision that is worse than 20/40 (dependent on foveal involvement), central and paracentral scotomas, and metamorphopsia.2,7 Anterior segment findings, although not as common, can consist of corneal punctate epitheliopathy and superficial iris atrophy.7 Initial posterior segment signs commonly include irregular pigmentary changes due to retinal pigment epithelium disruption and delineated yellow and grey lesions at the macula that coincide with the area of phototoxic injury, just as our patient presented.8,9,9 The posterior segments lesions can also take on an appearance that includes vertical and horizontal streaking rather than a focal location. Xu et al. described five patients that presented with a characteristic dendrite-like pattern, containing streaks that branched from the center of the foveal lesion. They suggested that the pattern was most likely due to micro saccades made by the eye when focusing on the laser pointer.7 Some cases have reported that these dendritic streak lesions are more commonly present in self-inflicted laser injuries compared to focal lesions seen in injuries caused by a third party.2,9 In the following months the retina can recover and regenerate however lasting retinal pigment epithelium changes/scarring may be seen as well as ellipsoid zone loss and cavitation.4–7 Other posterior segment findings that were not seen in our patient but have been reported in the literature include macular holes and retinal hemorrhages that can present in any location: vitreous, subhyaloid, intraretinal, and subretinal.1 Other findings can include cystoid macular edema (CME), epiretinal membrane (ERM) formation, and rarely choroidal neovascularization (CNVM) which can occur months to years after the initial laser pointer trauma.3,11,13 This underscores the need to monitor patients on a frequent basis.
Management of laser pointer maculopathy depends on the retinal presentation and sequela. In some cases, if macular holes are present, they can resolve on their own, but if they persist and enlarge then a pars plana vitrectomy may be needed.2,2,3,10 Other complications mentioned earlier can include vitreous hemorrhaging and retinal hemorrhages in varying layers. These can usually be observed as they tend to resolve without treatment.1 CME and ERM’s can also be monitored depending on if the location is non foveal. Surgical intervention is warranted if the degree of visual disability is large.9 Rarely patients can develop CNVMs. This is thought to be due to the laser damaging the outer blood retinal barrier, leading to inflammation and ischemia with resulting vascular endothelial growth factor release and angiogenesis.23 In limited cases reports in the literature these secondary CNVMs were treated with anti-vascular endothelial growth factor injections with favorable results.13,24,25 Lastly there have case reports and series that advocate the use of oral steroids for laser retinopathy. The laser is thought to induce an inflammatory response that is lessened by use of the steroids. Unfortunately, there has not been enough research to determine its clinical usefulness with most cases in the literature being anecdotal.1,1,2,7 In the absence of these complications, prognosis is generally favorable as long as there is limited or non-foveal damage.2,3,10 Most patients tend to naturally recover and visual acuity can improve over weeks to a few months. However, patients may still have persistent long-term visual distortion or scotomas secondary to irreversible retinal damage.2,9 Therefore the most appropriate management of patients presenting with laser pointer injury involves educating the patient, as well as their family, of the adverse ocular effects of laser pointer viewing.2 Furthermore, dilated comprehensive eye examinations should be performed annually to monitor for possible complications, such as CNVM, secondary to the laser induced trauma.
CONCLUSION
Laser pointer retinopathy is an increasingly prevalent condition in pediatric and adolescent patients due to ease of laser accessibility through online stores and limited knowledge of their dangers. This case demonstrates how children and teenagers can be unaware of the harmful visual complications of laser viewing, as it can go undiagnosed for years before being uncovered during a routine eye examination. Although the prognosis is favorable in a majority of cases, some cases have result in serious vision loss. As there is no truly effective treatment available awareness and education of laser pointers is vital. Optometrists can play an important role by informing and educating caretakers, parents, teachers and children about safe laser handling precautions and their potential to cause devastating ocular effects if mismanaged.
CE NOTIFICATION
This article is available as a COPE accredited CE course. You may take this course for 1-hour credit. Read the article and take the qualifying test to earn your credit. Click here to Enroll
Conflicts of Interest
The authors have no direct or indirect financial interest