Introduction
Optociliary shunt vessels (OSVs) are vascular loops that represent a communication between the central retinal vein and peripapillary choroidal veins in the prelaminar region of the optic nerve. Normal anatomical vasculature allows the central retinal vein to drain venous blood into the cavernous sinus. In optic nerves with OSVs, these vascular loops enable bypass of the retinal venous blood from an occluded central retinal vein through to the choroidal circulation. These vessels are thought to appear as a protective mechanism for the reperfusion of an ischemic retina from an ischemic event.1 Occlusion of the central retinal vein may either allude to a compressive lesion on the optic nerve or the aftermath of a vascular event. On fundus examination, these peripapillary vessels overlay the optic nerve and appear dilated, tortuous, and distinct from typical retina vascular branches.2 These vascular loops tend to present as a result of optic nerve sheath meningiomas (ONSM) but may also be associated with central retinal vein occlusions, chronic glaucoma, chronic papilledema, optic nerve drusen, optic nerve glioma, arachnoid cyst of the optic nerve, and phakomatosis.3,4
Retinal collateral vessels and neovascularization of the disc (NVD) are oftentimes mistaken for optociliary shunt vessels. Collateral vessels develop from within existing retina capillary networks in instances when a vessel becomes occluded but its adjacent vascular channels are still patent and functioning.2 They are also primarily located within the retina in comparison to OSVs located on the optic nerve itself. There are three types of collaterals that have been reported: arterio-arteriolar (A-A) occurring after a branch artery obstruction; veno-venular (V-V) occurring after a venous obstruction; arterio-venous (A-V) occurring during a capillary bed obstruction.2,3 Regardless, collaterals can be discerned from OSVs because they usually transpire from haemodynamic factors and altered blood flow in comparison to complete venous occlusion seen with shunt vessels.2 With regard to neovascularization of the disc, these typically appear as fine, net-like vessels that occur as a result of ischemia, most commonly from diabetes. These lacey vessels can be discerned from OSVs by utilizing fluorescein angiography.2 NVD will leak fluorescein with diminished hyperfluoresence over time while OSVs will continue to show flow through the vessels with clear, uniform borders.
Although OSVs can be congenital in nature, they most commonly exist as a secondary occurrence. As such, we will highlight the necessary measures to properly investigate a new onset OSV. This systematic approach will provide the tools needed for eye care providers to distinguish optociliary shunt vessels from its mistaken counterparts and determine its respective management. No identifiable health information was reported in the following case report.
Case Presentation
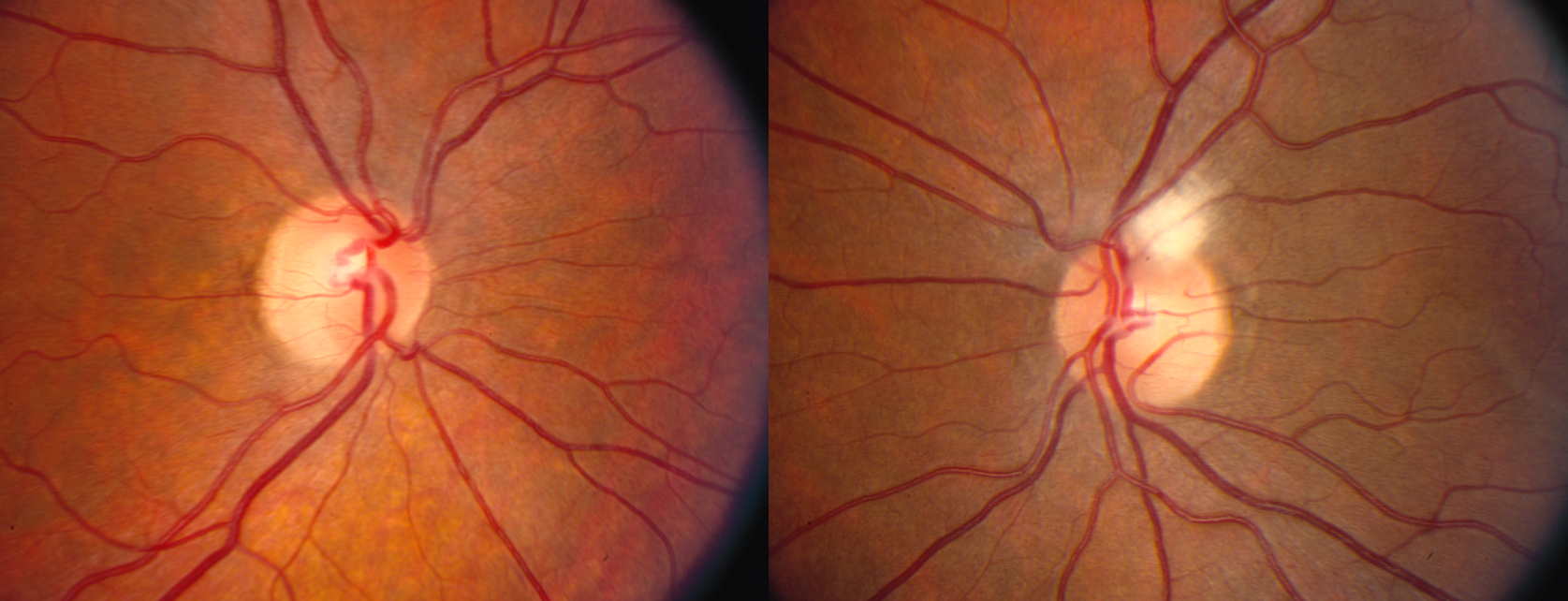
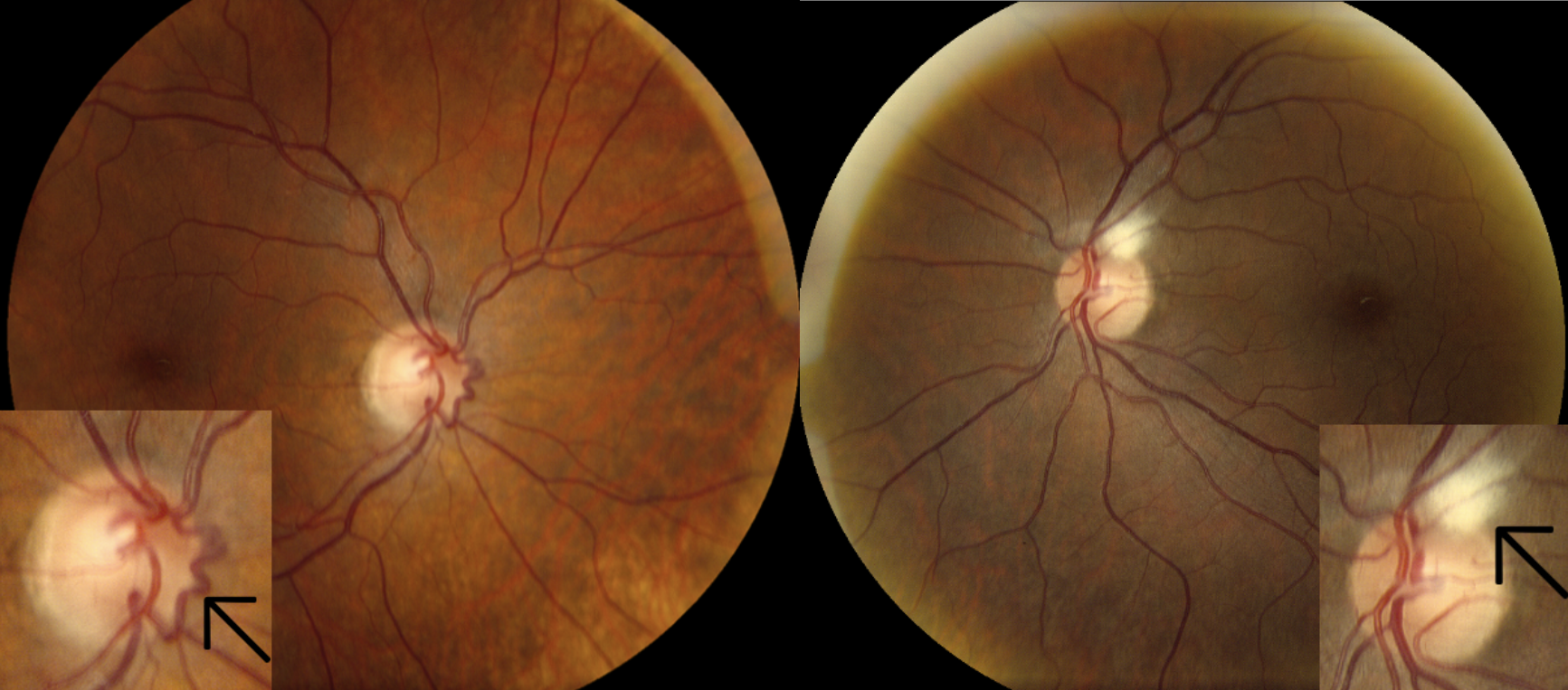
A 49 year old white female presented in 2012 for her annual comprehensive eye examination. Her initial chief complaints provided no relevance to the incidental finding of her optociliary shunt vessel. Ocular history was positive for myelinated nerve fiber layer OS and refractive error OU. Vascular systemic health was unremarkable. Best corrected visual acuity and all entrance testing were within normal limits. Fundus examination was pertinent for the following: optociliary shunt vessel vs collateral vessel OD, myelinated NFL OS. Refer to Figures I and II for fundus photos captured at her last examination in 2009 and in 2017 comparing the appearance of a newly acquired shunt vessel OD. No baseline photos were captured at the initial finding in 2012.


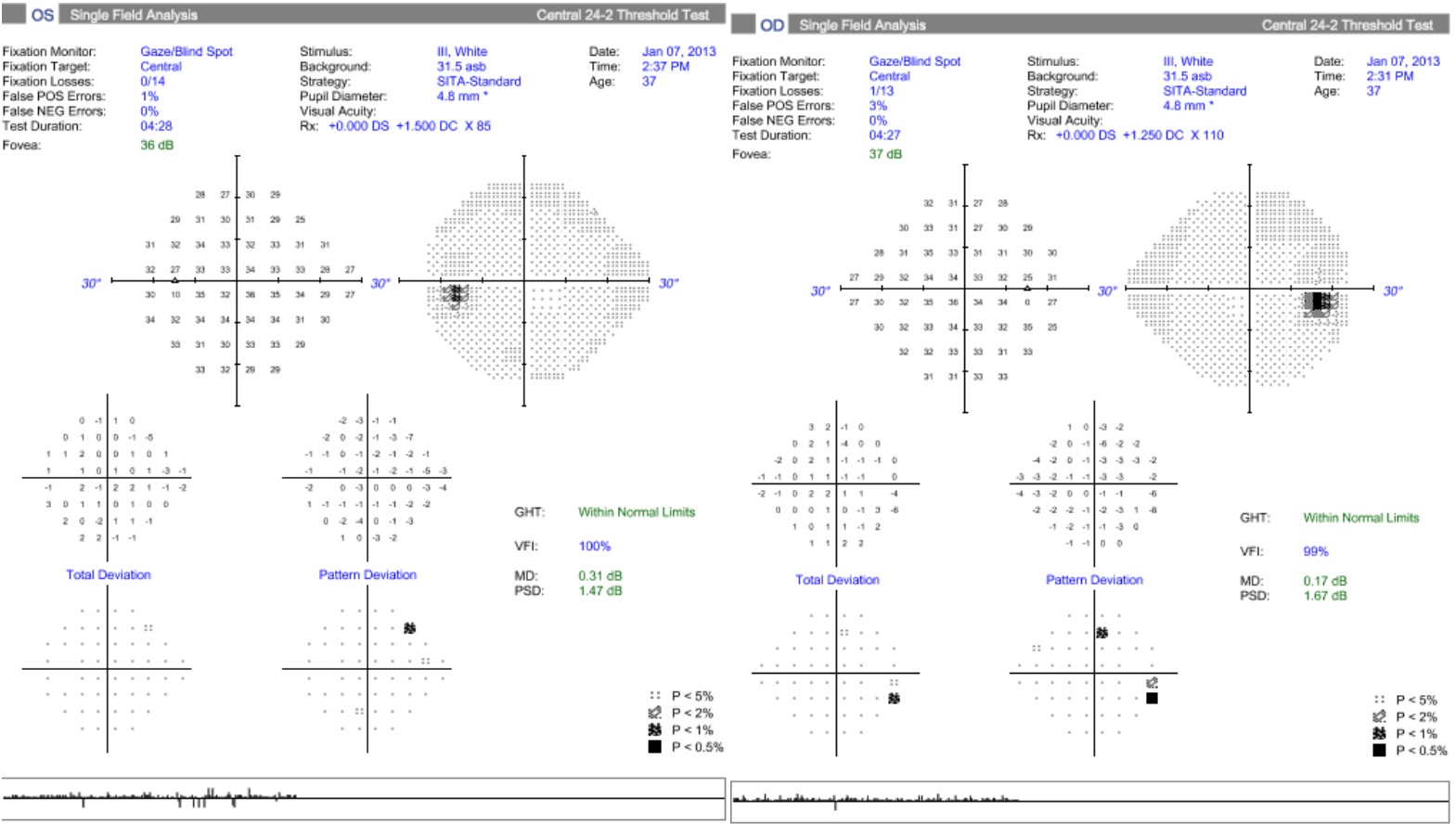
At this time, ophthalmology was consulted for further evaluation and recommendation. Due to the newly observed vascular loop, an MRI of the orbits was ordered to rule out optic nerve and retrobulbar abnormalities. Baseline Humphrey visual fields were also ordered which revealed non-neurological defects. See Figure III.

An MRI of the orbits with and without intravenous contrast was performed on 03/13/2013. Results showed “Normal MR orbits. No evidence of orbital mass.” The diagnosis of shunt vessel OD was given because an orbital mass was ruled out. To reiterate, the newly acquired shunt vessel finding in 2012 urged further investigation. There was also no evidence of glaucomatous optic neuropathy via OCT scans, visual field perimetry were full, and color vision was normal. Systemic health was unremarkable for vascular conditions. Once all ancillary testing returned normal, the patient was instructed to resume annual care in optometry with RNFL imaging as indicated.
Management and Outcome
Common differentials linked to acquired OSVs are listed in table I. As OSVs are often seen in conjunction with an ONSM, an MRI must be performed to rule out an orbital mass. While either a head MRI or orbital MRI is indicated for intracranial masses, an orbital MRI can provide better visualization of the optic nerve within the optic canal.5 A head MRI may not be the ideal modality as the cortical bone may cause lack of signal intensity which can further compromise proper evaluation of the optic nerve.5 As a result, MRI of the orbits tend to be the preferred imaging modality, however MRI of the head and/or CT scanning can still be utilized. Baseline Humphrey visual fields should also be performed to detect any functional loss from an orbital mass or chronic glaucoma.
Once neuro-imaging excludes an orbital mass, additional ancillary testing should be considered to help lead practitioners to the correct etiology. If vascular pathology is suspected, measuring blood pressure can give additional insight into uncontrolled hypertension which is a primary risk factor for retinal vein occlusions. If chronic glaucoma is suspected, patients should be managed accordingly as typical glaucoma suspects/patients without OSVs with serial RNFL scans and visual fields as deemed indicated. It is worthwhile to mention that although head imaging may rule out a mass, further research still needs to be conducted to rule in or rule out other common differentials for shunt vessels. In cases where chronic papilledema is suspected, the gold standard includes measuring intracranial pressure via lumbar puncture.6 Acceptable opening pressure in adults is ≤ 25cm H2O with higher than normal values confirming intracranial hypertension and subsequent papilledema.6 In cases where uncontrolled diabetes is suspected, optometrists should observe classic diabetic retinopathy findings, i.e., intraretinal hemorrhages, neovascularization of iris, disc, elsewhere, and exudative deposits, but should also be mindful of the recommended diabetic lab work-up to be completed by PCP. Primary eye care providers should do their due diligence to thoroughly examine each probable cause of newly developed OSVs.
Discussion
Optociliary shunt vessels can present as a congenital or acquired finding, although acquired is most commonly observed. Acquired shunt vessels were first reported in 1893 with limited reported literature thereafter.3 OSVs can also be recognized as “retinochoroidal veins of the optic disc”, “retinochoroidal venous collaterals”, “optociliary anastomoses”, and “retinociliary shunt/vessels” and are described as a variation of retina collateral vessels with some distinguishable features. Shunt vessels are described as a peripapillary vascular loop emerging from existing vascular anastomosis that runs from the central retinal vein to the choroid as a result of an ischemic event.3 These events may occur from compressive lesions, vascular conditions, chronic glaucoma, and chronic disc edema. These abnormal vascular loops are proposed to be a protective mechanism when retina ischemia happens to help circumvent other adverse ocular complications of ischemia, i.e., retinal neovascularization and associated sequelae.1
OSV outcomes from compressive lesions include ONSM, optic nerve glioma, arachnoid cysts of the optic nerve, and optic nerve drusen. ONSMs are benign, neoplastic lesions that originate in the optic nerve sheath and are considered the most common optic nerve tumor.7 As the tumor continues to grow, it will compress on the optic nerve which can cause a visual field defect and ultimately interfere with the blood supply to the optic nerve. When OSVs are present with a true ONSM, the clinical triad is observed as optociliary vessels, disc pallor, and reduced vision.8 Proptosis and an afferent pupillary defect may also be present.8 In these instances, a tumor is highly suspicious and a prompt MRI needs to be performed. Meningiomas are three times more prevalent in women than men, occurring in those ages 35-60 years old.7 Next, optic nerve gliomas are relatively rare tumors that typically present during childhood and have some association with neurofibromatosis type 1.9 If optic nerve gliomas occur during adulthood, they tend to be aggressive and usually leads to blindess and death. Much like ONSMs, the presence of a space-occupying mass will press on the optic nerve and cause devastating outcomes. Similarly, arachnoid cysts of the optic nerve are a benign distention and proliferation of normal fibrovascular tissue that comprises the leptomeninges which surround the optic nerve.10 It is thought to occur as a result of trauma, although the pathogenesis is not confirmed. These compressive cysts can also mimic optic nerve neoplasms and cause visual insult. The difficulty with distinguishing amongst these varying masses emphasizes the importance of performing neuro-imaging. Lastly, optic disc drusen are calcified deposits that are “buried” during childhood and become superficial as the patient ages. Visual acuity is typically spared with the potential for the visual field to become compromised. When these calcified bodies compress and constrict the optic nerve blood supply, OSVs may occur.
If MRI/CT imaging confirms presence of a mass, urgent referral to ophthalmology and neurology must be made. Current literature does not provide a universal treatment plan towards treating these lesions. Traditional approach usually includes observation until the eye is blind from tumor expansion at which continued observation may be done or complete tumor and optic nerve removal to relieve proptosis, pain, and intraocular complications.7,9 Surgical resection is an option, however there is a high recurrence rate of 21%.9 Radiation therapy has also been attempted with reported regression of the OSV.
If compressive lesions are excluded from neuro-imaging, optometrists should immediately suspect chronic and/or resolved retinal vein occlusions as OSVs occur in 30-61% in eyes with CRVO.1 Diabetic retinopathy also comes to mind, although the former is generally the primary cause. Investigation for potentially uncontrolled hypertension or diabetes should be conducted.
When suspecting vascular etiology, it is essential to note that OSVs may be the only clue to a chronic and/or resolved CRVO as opposed to the classic acute “blood-and-thunder” appearance. Kanai et al confirms the presence of an optocilary shunt vessel as actually beneficial since it improves visual prognosis in eyes with CRVO.11 When the central retinal vein is unable to properly drain venous blood through typical means, OSVs will form to create an alternate route via choroidal circulation.1 These vessels are able to bypass the site of occlusion and provide additional retina perfusion. Shunt vessels can develop 3-14 months after the initial vein occlusion.7 In addition to shunt vessels, both neovascularization of the disc and collateral vessels can also occur within vein occlusions and diabetic retinopathy.2 The key is to be able to differentiate between the three. Neovascularization of the disc appears as tufts of fine vessels that can proliferate into large fronds. These irregular vessels occur as a result of some hypoxic stimulus or nutritional deficit. As mentioned earlier, collateral vessels result when a vessel within the capillary network is occluded, yet its neighboring channels are still functioning properly.2 Over time, the collateral may adopt the same caliber and cellular characteristics as the vessel it replaced. Collaterals can even disappear if the obstructed vessel reopens. One identifiable characteristic between collateral vessels and neovascularization is that collaterals will possess true laminar flow during fluorescein angiography in contrast to hyperfluorescent leakage in neovascularization. Given the potential for underlying systemic conditions, optometrists should alert primary care for further evaluation.
Chronic glaucoma is another differential to be considered. Glaucomatous damage results from a pressure discrepancy between intraocular pressure (IOP) and intracranial cerebrospinal fluid pressure (ICP) at the lamina cribrosa (LC).12 This pressure gradient at the LC is also known as the translaminar pressure gradient (TLPG). There is a general consensus that lower ICP causes an unequal TLPG which produces additional strain at the LC. The reason for shunt vessel formation from chronic glaucoma proposes that elevated intraocular pressures creates a stasis in the central retinal vessels and subsequent vessel distortion.12 This same process can also be applied in instances with CRVO since there is increasing IOP buildup from compromised venous drainage. The difference with glaucomatous optic neuropathy is that we also see this strain causing the typical optic nerve cupping as the LC marginally moves away from the globe.12 Much like typical glaucoma patients, structural changes such as OSVs as a result of chronic glaucoma are slow to form. Baseline RNFL scans and visual fields should be completed with initiation of therapeutic intervention if indicated.
It is important to highlight that chronic papilledema can produce OSVs. The chronicity, including many weeks to months, ultimately leads to atrophic nerve fibers which result in severe visual impairment.12 Over time, the edema recedes and disc pallor will form. When this happens, the ICP remains elevated and forms shunt vessels as a response to the subsequent induced strain on the central retinal vein.
Absence of a mass, lack of correlating systemic vasculopathic conditions, normal intraocular pressures, and nonexistent disc edema led us to rule out the most common differentials. Retrospective chart review suggests presumed retina ischemia as our leading differential. In Figure I, the nasal retina vein wrapping above the first bifurcation of the inferior nasal artery is noted; it then passes underneath one of the subsequent branches creating a corkscrew appearance. This unique anatomical variation has led us to believe that an impingement between the artery and vein advential sheath has created the retinal ischemia responsible for the formation of the OSV in our patient. As seen in Figure II, the OSV appeared in its’ identical location, implying preexisting compression between this particular vein and artery.
Depending on the etiology, patients may or may not be symptomatic. In our case report, we discussed a new onset OSV in a relatively healthy 49 year old female with no visual or ocular symptoms. Visual acuity and all entrance testing were within normal ranges. Neuro-imaging results confirmed no presence of an orbital mass. Her ocular and systemic history lacked pertinent vascular conditions: she did not have diabetes, hypertension, or other significant comorbidities. Visual fields and RNFL scans all returned within normal limits without signs of glaucomatous optic neuropathy. After a complete and thorough work-up, no subsequent damage to the optic nerve has been seen since 2013. Therefore, the patient was recommended to maintain annually follow-up care with optometry.
Conclusion
Optociliary shunt vessels can be classified accordingly as congenital or acquired, although it is far more common to be acquired in nature. These acquired vessels are often an incidental finding during routine examination, highlighting the crucial role of optometrists in their ability to identify and manage the underlying etiologies. As orbital masses are the primary suspected etiology, timely investigation and neuroimaging are imperative. Systemic vasculopathic conditions and chronic glaucoma are also significant differentials which require ongoing management by primary care physicians and optometrists, respectively. As primary eyecare providers, optometrists are responsible for detecting potentially vision and life-threatening conditions in seemingly asymptomatic patients. The proper identification, investigation, and management of OSVs are crucial steps in ensuring optimal patient care and preventing severe complications.