
Introduction
Silver, a naturally occurring element, has long been used for various applications due to its multiple valuable physical properties including high thermal and electrical conductivity, malleability, and ductility.1 Prolonged exposure can result in the accumulation of silver in skin, mucous membranes, and internal organs, which may subsequently lead to argyria, a rare dermatological condition.2,3 The deposition of silver in the eye and periocular tissue is specifically known as ocular argyrosis. This clinically presents as gray-blue discoloration of the periorbital skin, bulbar and palpebral conjunctiva, and lacrimal sac. Corneal opacities within Bowman’s membrane, the stroma, and Descemet’s membrane, and cataracts have also been reported.3–5
Ocular argyrosis may be associated with occupational exposure, long-term ingestion of silver-containing medicinal solutions, and prolonged application of silver-tinted makeup products.6–9 Though not commonly observed, there has been a resurgence of silver-containing products in alternative medicine that may potentially lead to silver toxicity.10
The diagnosis of ocular argyrosis is determined through clinical presentation and diagnostic testing using multimodal ocular imaging and can be confirmed through investigative methods including serum silver levels and conjunctival biopsy.11
In this case report, we describe the initial presentation of bilateral early drusenoid changes within the macula in each eye that was found on routine comprehensive eye examination in a 75-year-old patient that had been chronically ingesting his own concoction of colloidal silver. We review updates on the clinical manifestations and ancillary testing of ocular argyrosis.
Case Report
A 75-year-old Caucasian male presented with a chief complaint of dry eyes. He also noted that overall, his vision had appeared to improve in the past few years due to his ingestion of self-concocted colloidal silver solution. His personal ocular history was significant for dry eye syndrome and cataracts.
The patient’s medical history was significant for liver cirrhosis, osteopenia, elevated PSA, marijuana abuse, benign prostatic hyperplasia, saccular aneurysm, microscopic hematuria, hemospermia, pilar cyst, generalized anxiety disorder, chronic post- traumatic stress disorder, and hepatitis C. He reported chronic ingestion of silver colloid of various concentrations, which he began in 2006 in the hopes of curing his multiple medical ailments. Through information gathered from several online social media groups, he created his own concoctions using a silver generator and silver strips. He took it daily for approximately a year, experimenting with extremely high concentrations and dosages ranging from half a liter to a full liter. He had been followed by dermatology due to a spot of cancer on his nose and was formally diagnosed with argyria a few years ago. He currently drinks on average 12 ounces of the silver concoction daily.
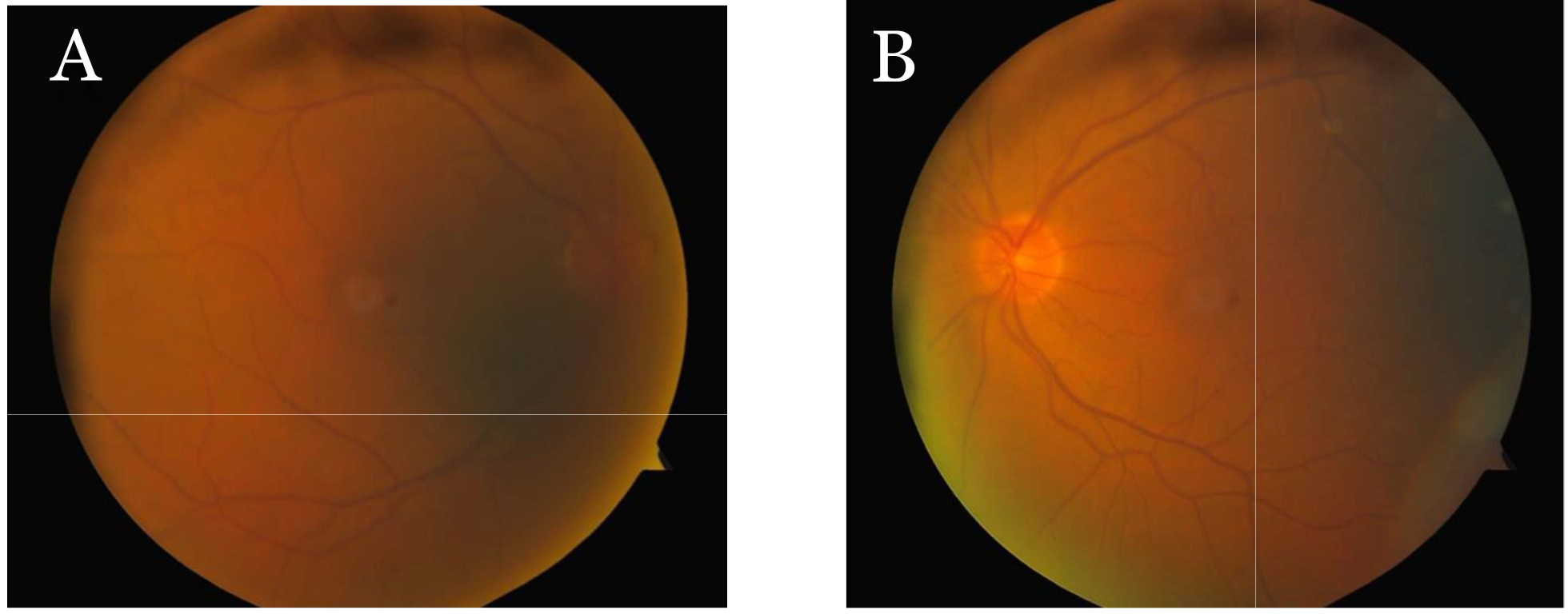
_right_eye__(b)_left_eye.png)
Best corrected visual acuity was 20/20 OD and 20/20 OS. Extraocular motility testing revealed full and smooth eye movements without any restrictions. Confrontation visual fields were full to finger counting OD/OS. Pupils were round and equally reactive to light, with no relative afferent pupillary defect noted.

Slit lamp examination was remarkable for 2+ capped, inspissated Meibomian glands and 1+ injection. The tear break-up time was found to be instantaneous in each eye.
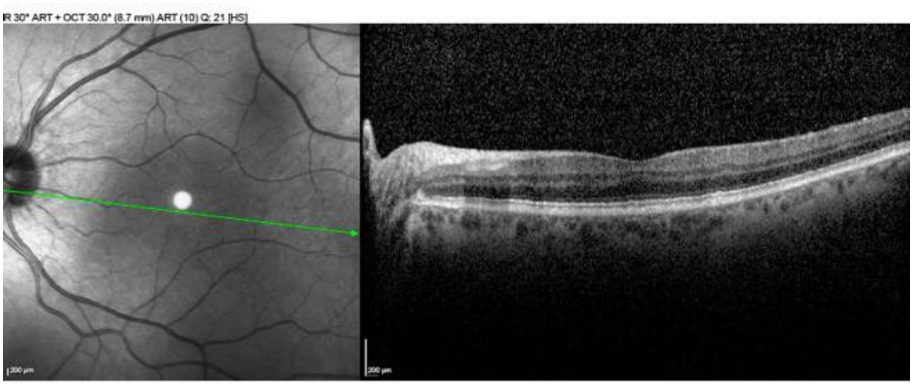
Goldmann applanation tonometry (GAT) measured 12 mmHg OD/OS prior to dilation. Pachymetry measured 515 um OD and 512 um OS. Fundoscopy revealed cup-to-disc ratios of 0.30 rnd OD/OS and the initial presentation of mild to moderate drusenoid changes concentrated superiorly to the fovea OD and temporal/inferior temporal to the fovea OS. Spectral-Domain Ocular Coherence Tomography scans of the macula demonstrated a few scattered perimacular drusenoid deposits, localized to the inner segment ellipsoid layer.
The patient was diagnosed with ocular argyrosis and recommended to discontinue consumption of silver solution. A strict regimen of dry eye treatment including artificial tears, good lid hygiene, and warm compresses with lid massage was prescribed.
Systemic lab testing was ordered and revealed slightly elevated silver serum levels of 5.7 mcg/L (<5 mcg/L).
Discussion
Ocular argyrosis is a rare condition that can occur secondary to chronic exposure to silver compounds through ingestion, inhalation, or skin contact. Exposure hazards include working with silver compounds in an occupational setting, self-application of silver-tinted makeup products, or chronic use of topical silver colloid solution.11,12
Excessive intake of silver can lead to the deposition of silver in various internal organs, with the highest concentrations found in the skin, liver, spleen and adrenal glands.13 It can be either asymptomatic or result in discoloration of the affected tissues.14 The pathophysiology is still not completely well-understood though this process has been studied in detail. In generalized argyria, silver particles can form complexes with protein, DNA, and RNA molecules as they are absorbed in the bloodstream. The particles travel throughout the body, resulting in their deposition in a variety of tissues including the ciliary body and choroid. The longer the duration of silver nitrate administration, the greater the amount of silver accumulated in basement membranes.11
Ocular signs of argyrosis manifest primarily as discoloration of the affected basement membranes and alterations in both anterior and posterior segment including the eyelids, conjunctiva, cornea, lens, ciliary body, and Bruch’s membrane (Table 1).5
The rarity of this condition may not lend itself to immediate recognition. Differential diagnoses to consider when confronted with observations of clinical signs and symptoms include other keratopathies, heavy metal deposition, conjunctival pigmented lesions, and, in the presence of retinal changes, age- related macular degeneration.15
Comprehensive multimodal ocular imaging can assist in the diagnosis of silver deposition in various ocular tissues. Anterior segment ocular coherence tomography (AS-OCT) and confocal microscopy has confirmed the presence of silver granules especially in the cornea, presenting as a hyper-reflective Bowman and Descemet’s membrane.16,17 Of particular interest is the observation of bilateral confluent drusenoid deposits that can be confirmed with spectral- domain ocular coherence tomography (SD- OCT) as well as choroidal thinning captured by Enhanced Depth Imaging (EDI-OCT).2,18
Conclusion
Colloidal silver has traditionally been promoted as a cure-all for various ailments and has more recently made a comeback in alternative medicine in the protection against and treatment of conditions including COVID-19. The inherent therapeutic properties in modern preparations of silver nanoparticles, with their antiviral, anti-inflammatory, and wound-healing effects, have also garnered increasing interest due to their potential biomedical applications. Further research is necessary to investigate the systemic absorption of colloidal silver and its adverse effects. As demonstrated with this case, a detailed history and examination is imperative to determining the underlying etiology and differentiating similar ocular manifestations. With the current lack of effective treatment options, early diagnosis and prevention of overexposure are crucial.
_right_eye_(b)_left_eye.png)