Introduction
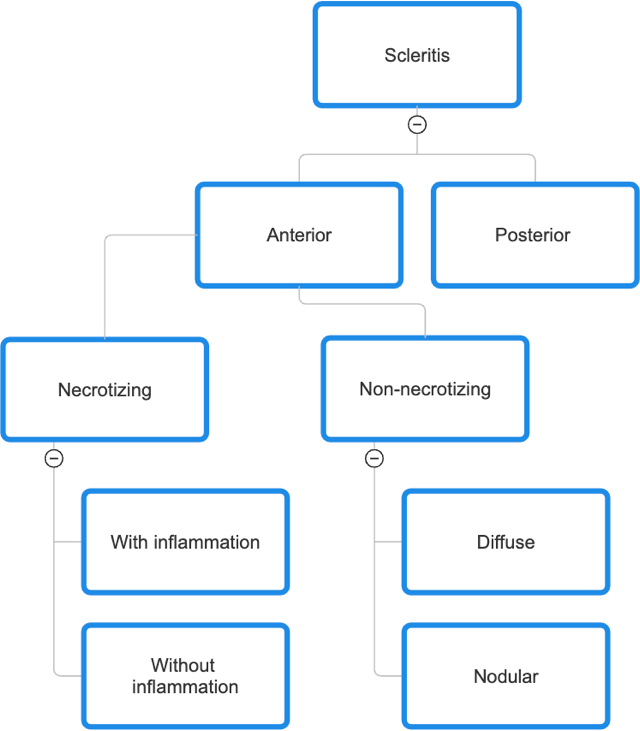
Scleritis is a pathological condition characterized by inflammation of the sclera, which is the outermost layer of the eye. Scleritis can be classified into different categories, namely anterior (including non-necrotizing diffuse or nodular and necrotizing with or without inflammation), posterior, and infectious. In contrast to episcleritis, scleritis poses a risk to vision and is potentially sight-threatening. Furthermore, approximately 50% of scleritis cases are linked to systemic diseases, with the severity and manifestation of the disease playing a significant role in this association.
Case History
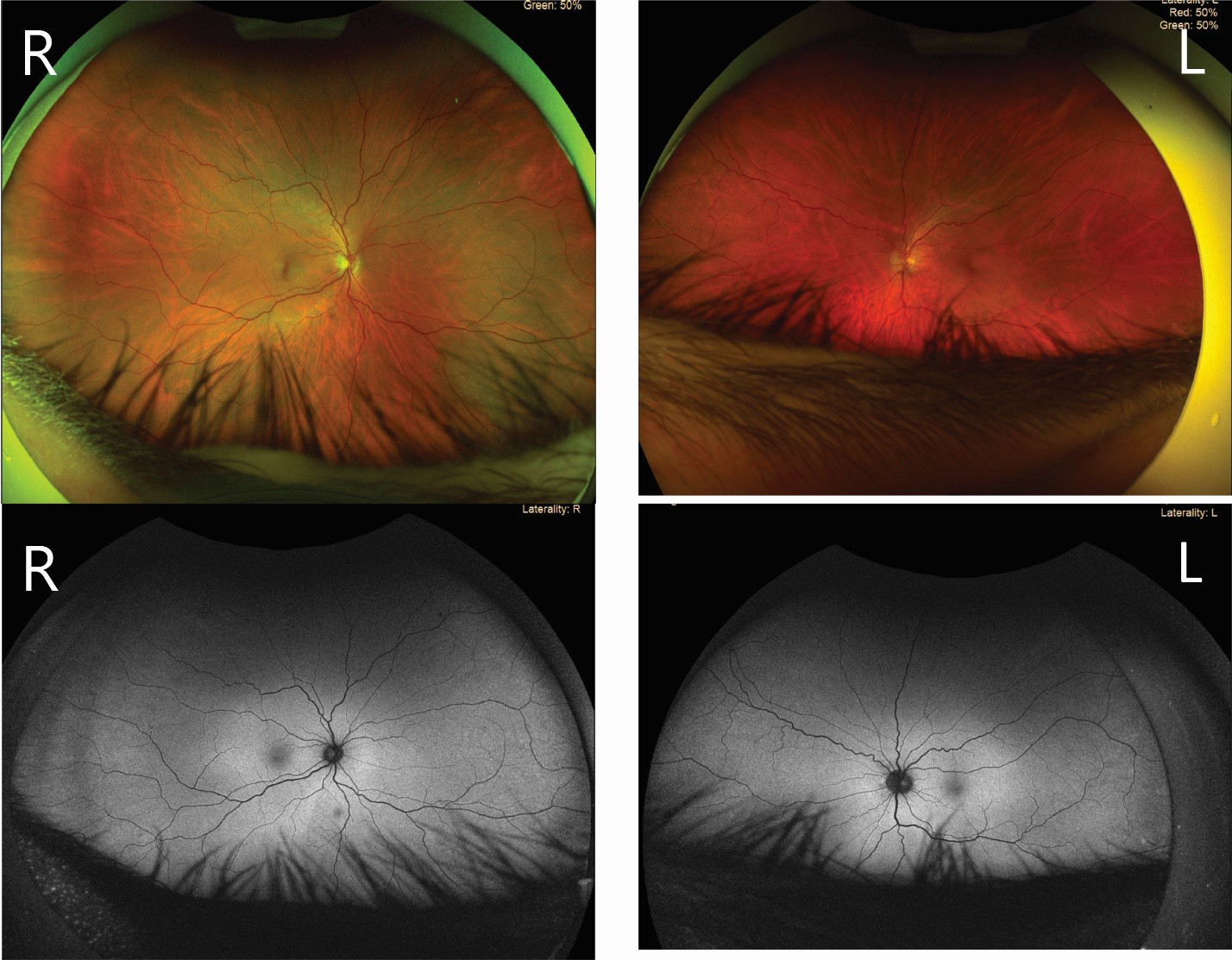
A 46-year-old Caucasian male presented for an urgent eye examination on October 28th, 2023, due to a red, watery, and painful right eye that started on October 27th. Ocular history was remarkable for LASIK in both eyes in 2021. He noted no previous occurrence of trauma or infection to his eyes and that this was the first episode. Medical history included questionable hypothyroid, still being monitored by the family doctor, with no other conditions of note. No allergies to drugs were mentioned.
Unaided visual acuities were 20/20 in each eye. Pupils were equal, round, and reactive to light, with no RAPD. Extraocular motilities revealed no restrictions, but he did note pain upon eye movement. Intraocular pressure @ 1:28 PM was 12mmHg in each eye. Palpation of the adnexa noted mild tenderness of the right eye. No preauricular lymphadenopathy and skin lesions were noted.
Anterior segment examination revealed mild tenderness of the right eye and around the adnexa. In addition, 4+ bulbar hyperemia, 3+ hyperemia of the inferior palpebral conjunctiva, and 3+ conjunctivochalasis of the right eye were noted. No follicles, corneal infiltrates, edema, or corneal epithelial defects were noted. All else was within normal, and the left eye was unremarkable. After instillation with phenylephrine 2.5%, blanching of the temporal conjunctiva was noted with persistent hyperemia of the nasal quadrant.

Differential diagnosis
-
Simple diffuse episcleritis
-
Episcleritis refers to the inflammatory condition affecting the episclera.1The episclera, composed of connective tissue, is situated in the intermediate space between the conjunctiva and sclera. Young adult females are the main demographic affected by the condition, and idiopathic cases account for most instances.1,2
-
The signs and symptoms of this condition encompass gentle ocular discomfort or pain, excessive tearing, sudden start of redness in the eye, and slight soreness.1,2 Visual acuity often remains unaffected.
-
The application of a 2.5% phenylephrine solution induces constriction of the conjunctival and superficial episcleral plexus vessels, resulting in a blanching effect.1 In this particular instance, the hyperemia exhibited by the patient did not fully diminish upon administration of phenylephrine. This suggests the deep vascular plexus was also involved in the observed condition.
-
-
Conjunctivitis
- Papillae are predominantly observed in cases of allergic or bacterial conjunctivitis.3,4 Nevertheless, it is worth noting that bacterial conjunctivitis seems to be more prevalent among pediatric populations compared to adults.5 Neisseria gonorrhoeae, a prevalent etiological agent of bacterial conjunctivitis in sexually active individuals, commonly presents with the presence of tender and palpable preauricular lymph nodes (PAN), discharge, and stuck eyelids in the morning.5,6 The absence of the aforementioned signs in the patient’s examination findings rules out the possibility of bacterial conjunctivitis as a diagnosis.
-
Viral conjunctivitis commonly exhibits interocular transmission. The diagnosis was excluded as the patient had a notable degree of unilateral conjunctival edema and scleral hyperemia. Furthermore, the individual did not exhibit the presence of follicles, which is a characteristic manifestation of viral conjunctivitis.4
-
Allergic conjunctivitis commonly manifests bilaterally with a reduced presence of hyperemia. In addition, it is important to note that allergic conjunctivitis does not elicit pain in response to ocular motion, and it commonly manifests bilaterally rather than unilaterally.2 Typical manifestations of allergic conjunctivitis commonly encompass a medical background of allergies or atopy, pruritus, and the absence of preauricular lymphadenopathy.2
-
Anterior diffuse scleritis
- Symptoms of the patient: moderate/severe pain, pain upon eye movement, light sensitivity, epiphora, unaffected visual acuity, and persistent hyperemia after instillation of 2.5% phenylephrine all suggested a working diagnosis of anterior diffuse scleritis.
Working diagnosis: Anterior diffuse scleritis of the right eye
He was prescribed prednisolone acetate 1.0% ophthalmic suspension four times a day and was instructed to take naproxen sodium capsules (220 mg) 2 tabs twice a day. He was cautioned regarding the gastrointestinal side effects of taking a non-steroidal anti-inflammatory drug (NSAID). A follow-up examination was booked for October 30th (2 days) to follow up on his symptoms.
Follow-up 1 (October 30th, 2023)
On the two-day follow-up appointment, he noted that the pain had subsided to mild soreness and irritation with a reduced hyperemia upon observation. He reported using seven drops of prednisolone acetate 1.0% ophthalmic suspension since his last examination and did not take naproxen sodium capsules (220 mg) as instructed. All other entrance testing was the same as day 1. Intraocular pressures @ 2:38 PM were 16 mmHg and 15 mmHg. Blood pressure (in- office, brachial auto, sitting @ 2:38) was 141/92 mmHg with a heart rate of 62 bpm.
Anterior segment examination revealed no tenderness upon palpation around the eyelids and adnexa with 2+ bulbar hyperemia nasal, trace hyperemia temporal, 2+ conjunctivochalasis, and 1+ hyperemia of inferior palpebral conjunctiva in the right eye. The left eye was unremarkable. No dendrites, edema, or skin lesions were noted on this day. Dilated posterior segment examination was unremarkable.
He was then instructed to continue with prednisolone acetate 1.0% ophthalmic suspension QID and a prescription for naproxen sodium capsules (220 mg) 2 tabs twice a day. He was advised on the importance of medication adherence to help relieve his symptoms and aid the rate of recovery. He noted that he would see his family doctor on November 2nd for his thyroid. A letter of update to the family doctor was sent to rule out any systemic etiology associated with the anterior diffuse scleritis in the right eye.
Follow up #2 (November 7th, 2023)
On the ten day follow up appointment, he noted that there were no soreness or irritation. He was taking prednisolone acetate 1.0% ophthalmic suspension and naproxen sodium capsules (220 mg) as prescribed and reported adherence to schedule. All entrance testing were the same as previously noted. Intraocular pressures @ 9:13AM was 14 mmHg in each eye. Anterior segment examination revealed trace bulbar hyperemia nasal and temporal with trace conjunctivochalasis in the right eye. Left eye was unremarkable. It was discussed that his ocular condition has resolved. He was then advised to start tapering prednisolone acetate 1.0% ophthalmic suspension from QID to TID for 1 week, BID for 1 week and QD for the last week and continue to take naproxen sodium capsules (220 mg) for another week and then discontinue. A follow up was scheduled in a month to observe for any steroid response.
Discussion
Epidemiology and Pathophysiology
The sclera is composed of connective tissue, serving the purpose of safeguarding the ocular contents, resisting deformations, establishing a linkage with the extraocular muscles, and collaborating with the cornea in the precise focusing of light onto the retina.7 The sclera is anatomically linked to the cornea through the limbus. The fusion between the sclera and the dura of the optic nerve and lamina cribrosa occurs posteriorly.7 Similar to other types of connective tissue, the sclera is mostly composed of water and collagens, accounting for around 68% and 28%, respectively. Additionally, proteoglycans and elastin are also included in the composition of the sclera.7The orientation of collagen fibres varies to produce an opaque
appearance, in contrast to the transparent nature of the cornea.7 Despite their relatively small proportion, proteoglycans and elastin play a crucial role in the structure and function of the sclera. Proteoglycans play a vital role in the maintenance of fibril size and organization, while elastin is essential for ensuring structural integrity, form, and viscoelasticity.7
The sclera is composed of three distinct layers, namely the episclera, stroma proper, and lamina fusca.8,9 The episcleral layer is a thin layer of connective tissue that comprises a superficial episcleral plexus and a deeper vascular plexus.7,8 The biomechanical performance of the sclera is primarily governed by the stroma proper, which consists predominantly of type I collagen. The lamina fusca, also known as the suprachoroid, serves the purpose of connecting the sclera to the choroid.7,8
Scleritis can be mainly categorized into anterior and posterior types, with the insertion site of extraocular muscles serving as the distinguishing factor.9 The term “anterior” can subsequently be categorized into two subtypes: non-necrotizing and necrotizing. Non- necrotizing scleritis include both diffuse and nodular scleritis, while necrotizing scleritis can be classified as either with or without inflammation (Figure II).10

Anterior scleritis is the predominant form, which comprises 98% of reported cases. Within this category, anterior diffuse scleritis is the most often observed subtype, accounting for 45-61% of cases.9,11 Posterior scleritis, characterized by inflammation occurring posterior to the insertion sites of the extraocular muscles, constitutes around 2% of reported cases.9
Scleritis, an inflammatory condition characterized by painful inflammation of the sclera, commonly manifests in females aged 40 to 60 years.2,9,10 Previous research has documented that the prevalence of scleritis was 6 cases per 100,000 individuals in the year 2014. More recent investigations have reported an annual incidence rate of 5.54 cases per 100,000 individuals, with a higher tendency among females.12,13
Up to 39–48% of scleritis cases are linked to systemic diseases, despite the fact that many cases are idiopathic.11 Scleritis is commonly linked to various systemic conditions, such as rheumatoid arthritis (with a prevalence ranging from 6.4% to 15.2%), seronegative spondyloarthropathies (1.3% to 4.7%), inflammatory bowel disease (2.2% to 3.3%), vasculitides
(2.3% to 9.1%), systemic lupus erythematosus (2.0% to 4.1%), relapsing polychondritis (1.6% to 2.2%), and other less prevalent systemic diseases.14 Patients diagnosed with anterior necrotizing scleritis exhibit a greater propensity for systemic diseases (ranging from 45% to 95%) in comparison to those with posterior scleritis (ranging from 19% to 45%).11
Signs and Symptoms
Table I provides an easy-to-understand overview of the symptoms and signs associated with anterior and posterior scleritis.2,10 Scleritis is commonly identified by the presence of pain that is exacerbated by ocular movement and nocturnal periods, soreness, sensitivity to light, and hyperemia without any accompanying alterations in visual acuity.2,10 Furthermore, it should be noted that posterior scleritis is characterized by a reduction in visual acuity as a result of impairment to the optic nerve and the surrounding retina.15 Necrotizing anterior scleritis without inflammation, specifically scleromalacia perforans, is characterized by a distinct clinical presentation featuring minimal pain and redness. This condition is commonly observed in individuals with rheumatoid arthritis.11 Typically, indications of scleritis encompass scleral edema, tenderness of the globe, and the presence of large deep episcleral arteries that do not exhibit blanching when exposed to 2.5-10% phenylephrine.2,9,11 Additional findings may be present depending on the specific kind of scleritis, including the presence of an immovable nodule, changes in coloration, thickening of the posterior sclera, and the potential development of staphyloma and perforation.
Treatment
The initial course of treatment frequently involves the administration of topical corticosteroids and oral nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (400 – 600 mg) taken four times daily, naproxen (250-500 mg) taken twice daily, or indomethacin (25 mg) taken three times daily.2,10 Necrotizing scleritis, as well as instances of non-necrotizing scleritis that exhibit resistance to the aforementioned treatment, are managed by the use of oral corticosteroids as opposed to topical application. Alternatively, patients may be referred for immunosuppressive therapy and/or receive triamcinolone injections.16 While oral corticosteroids have demonstrated efficacy, their long-term use is constrained due to the presence of adverse effects.
Prolonged exposure to oral corticosteroids medications may result in a weakened immune system, making individuals more susceptible to opportunistic and bacterial infections.17 Additionally, they can have a detrimental impact on bone health, potentially leading to osteoporosis and fractures.17 Weight gain, particularly in the form of increased body fat, is a common side effect of long-term steroid use.18 Moreover, individuals may experience mood disturbances, such as anxiety and depression.19
Second-line therapies encompass the utilization of Anti-tumor necrosis factor (TNF) and biologic medicines, including Rituximab.16 These treatment options are advantageous as they mitigate the need for prolonged steroid therapy and specifically target the inflammation cascade.16 Table II presents an expansive list of first-line therapy options, categorized according to the specific form of scleritis that has been detected.
As previously mentioned, scleritis is frequently linked to systemic health conditions. Conducting an extensive physical examination is essential in order to identify an underlying diagnosis. In conjunction with an in-depth examination of the musculoskeletal, integumentary, and
cardiopulmonary systems, it is advised to run a blood analysis encompassing various parameters such as complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), uric acid levels, rapid plasma regain (RPR), fluorescent treponemal antibody absorption (FTA-ABS), rheumatoid factor (RF), antinuclear antibody (ANA), angiotensin- converting enzyme (ACE), and antineutrophil cytoplasmic antibodies (ANCA).9,11
CBC looks at the patient’s overall health, detecting anemia, infections, or blood disorders.20 ESR offers insight into the presence of inflammation.21 Uric acid levels are important for identifying gout.22 Serological tests such as RPR and FTA-ABS are essential for diagnosing syphilis.23 RF, ANA, ACE, and ANCA are vital in assessing autoimmune and rheumatological disorders.21
This patient did not mention any autoimmune, infections, or inflammation that may be the origin of his ocular condition. Therefore, a letter of update was included to the family doctor to rule out other underlying systemic aetiologies that were not noted before.
Conclusion
Scleritis is a condition characterized by a pronounced and vision-endangering inflammation of the sclera, which frequently presents notable difficulties in both diagnosis and treatment.
Without prompt identification and treatment, the inflammation has the potential to extend to neighbouring anatomical components, resulting in detrimental effects and ultimately causing a decline in visual acuity. The management of scleritis encompasses not only the administration of appropriate therapeutic interventions, but also the expeditious referral of patients to investigate potential systemic causes, such as rheumatoid arthritis.
Financial Disclosure
The author has no financial or proprietary interest in any material or method mentioned in this article.