Introduction
While it is recognized that the occurrence of a DH represents a risk factor for development of VF and RNFL loss, little is known regarding the series of underlying mechanisms that bring about these pathological changes.1–8 The development of new imaging technologies, however, has contributed to enhancing our comprehension of underlying etiological processes. Although LC defects are correspondingly associated with DH, they are not directly casually related. Similar indirectly related factors may give rise to their occurrence.9,10 The other etiological factors that may be considered include mechanical, vascular, and related retinal blood barrier dysfunction.11 Some investigators have indicated that reduced retinal metabolism associated with diminished neuro- retinal functionality may lead to reduction of peripapillary vascular density.12 This consequently may lead to changes at the optic nerve that may lead to the development of LC defects. In this case the pathology in glaucoma may not be restricted to changes affecting the optic nerve individually, but as suggested by other investigators, may involve forces affecting the homeostasis of all ocular structures.13 While the occurrence of DH will not necessarily lead to the development of VF loss in normo-tension glaucoma (NTG) evidence suggests that it may lead to subsequent RNFL loss that may precede VF loss.14,15 Other investigators have indicated that lowering (IOP) may reduce the rate of RNFL loss and be beneficial at reducing VF progression in glaucoma subjects that had optic nerve hemorrhages.1,16
Patients presenting with normal optic nerve appearance, low IOP, an antecedent DH and subsequent RNFL pre-perimetric loss represent a managing dilemma on commencing treatment. The purpose of this paper is to discuss a case with a long history of normal optic nerve appearance, and a preceding DH that developed pre-perimetric RNFL loss. A concise analysis and discussion of current evidence-based research utilized to justify this case management is covered in this paper.
Case Report
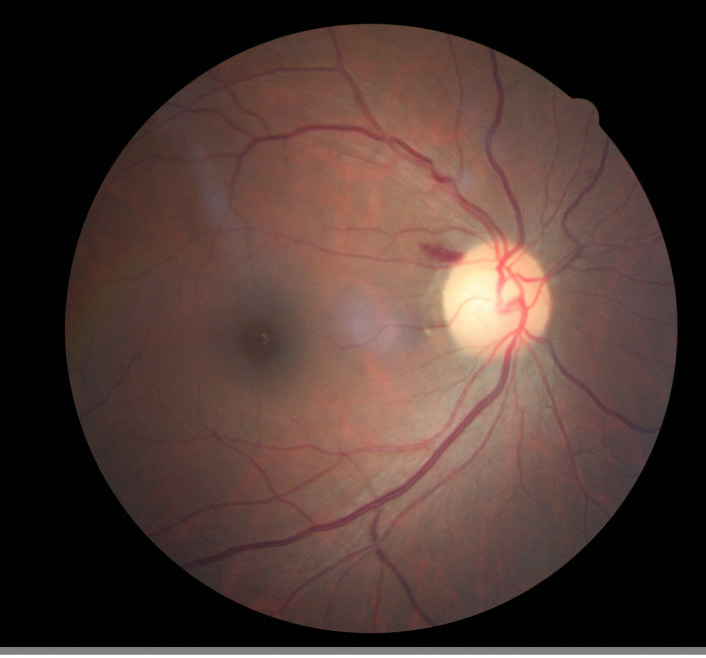
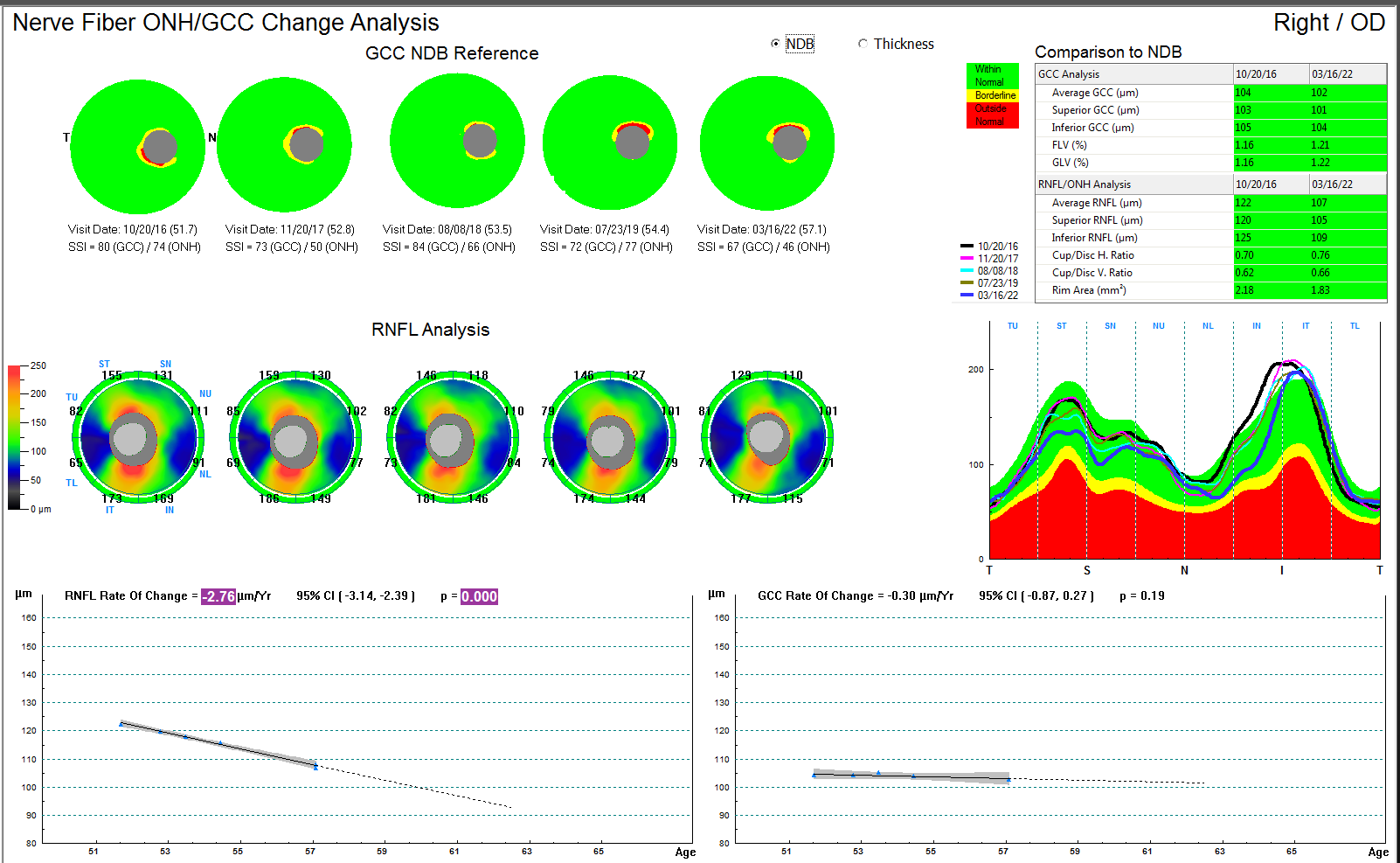
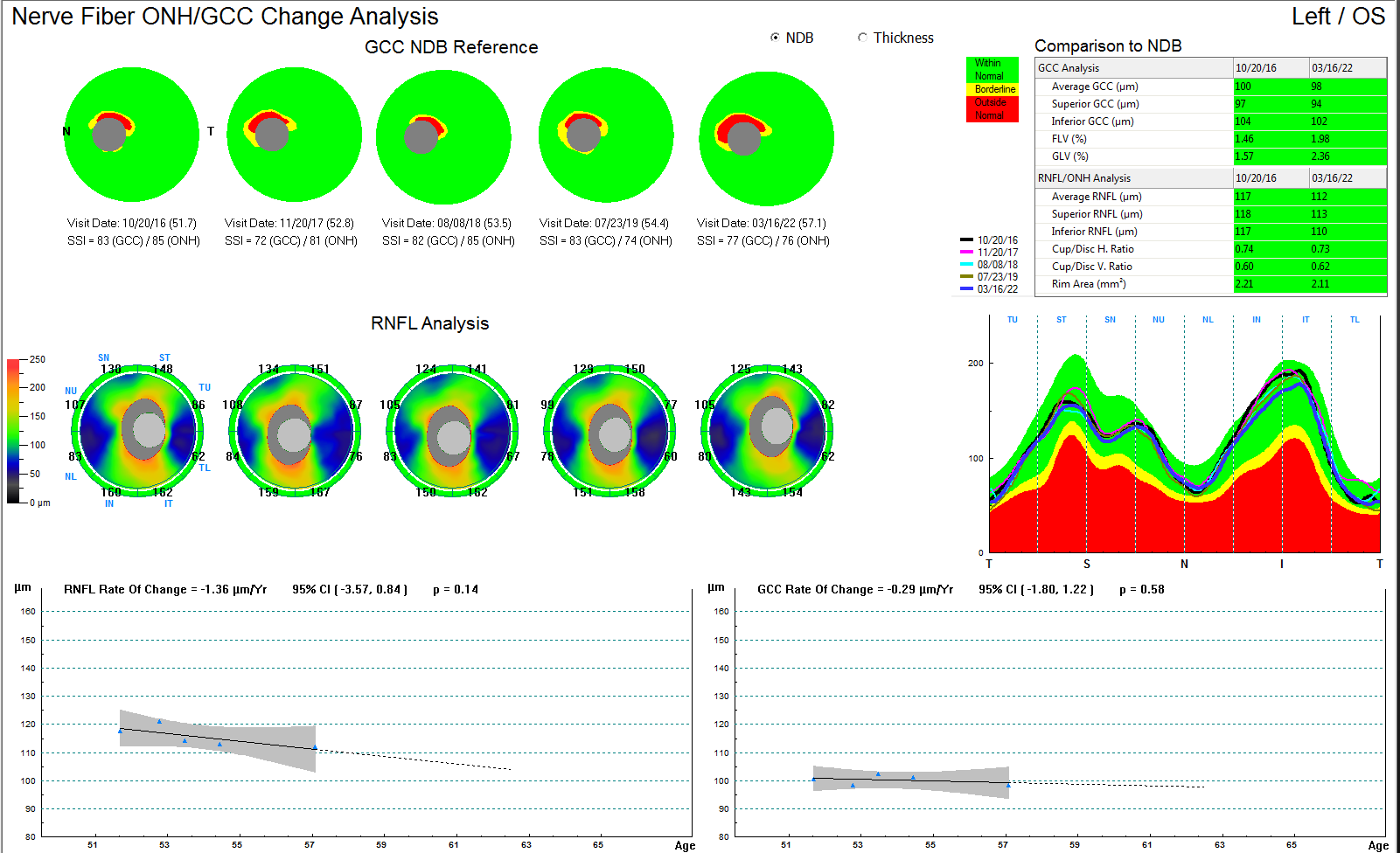
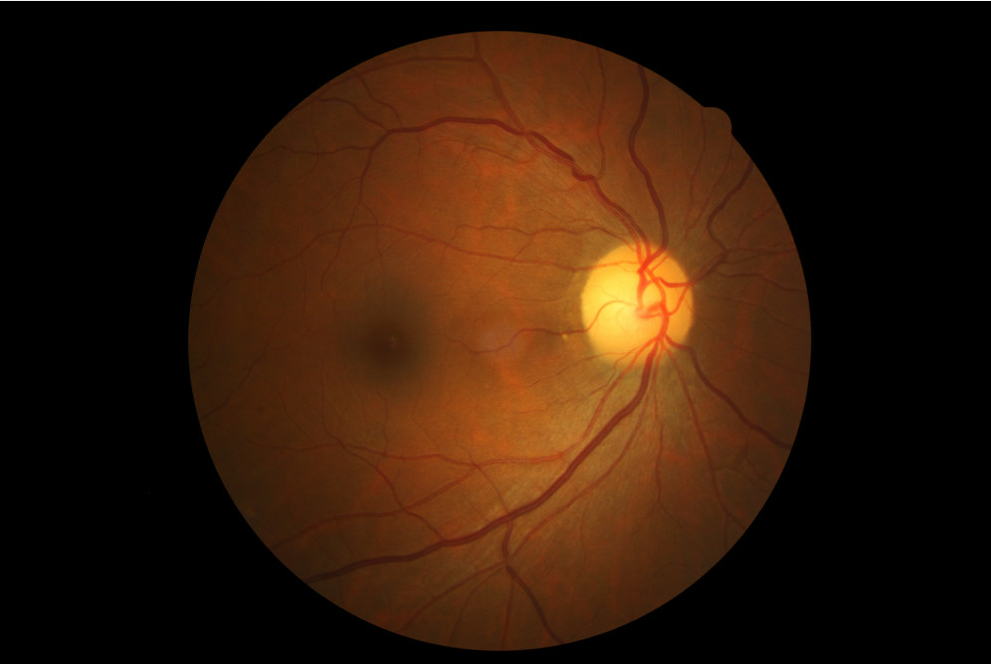
A 57-year-old female examined during a period of 5 years with generally unremarkable ocular findings, presented with a DH superior temporal on the disc rim tissue OD (figure1). The best corrected visual acuity was 20/20 OD/OS. Preliminary findings including pupil reaction were all normal. IOP ranged from 7 mm Hg to 13 mmHg during the previous 5 years and subsequently during follow-up visits, totaling 11 years. The cup/disc (c/d) ratio of 0.7/0.7 remained consistent with healthy rim tissue since the initial visit. A slit RNFL defect was however noticeable proximal to the superior temporal location of the DH (figure 1). The SDOCT and VF performed at the onset of the observed DH were both normal. Pachymetry values were 457 um OD and 443 um OS. At a follow-up visit approximately 3 years from the observation of the DH, RNFL loss progression was detected superior temporal corresponding to the previous DH quadrant location (figure 2). The SDOCT of the left eye was stable (figure 3). The DH was no longer present (figure 4). The RNFL rate of change for the right eye was -2.76 um/yr.


.png)

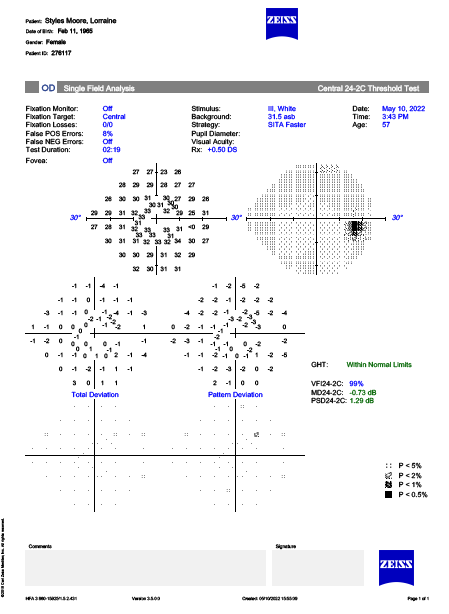
Estimation of conversion to glaucoma assuming 75 ums as the tipping inflection point of RNFL/VF loss in glaucoma17 for the average RNFL was approximately 12 years. VF testing remained normal OD (figure 5). Initiating treatment to lower IOP was not considered since the superior, inferior, and average RNFL measurements were 107, 109 and 108 ums respectively which was within the normal range. In addition, the estimated possible conversion to glaucoma was 12 years. A second opinion from Ophthalmology concurred with the assessment and it was recommended to continue close observation. However, if further progression was evident starting IOP lowering medication then would be considered.

Discussion
While a DH is known to occur in normal individuals, it is encountered predominantly in patients with NTG and to a lesser extent in those with higher IOP.3,8,11,14,18,19 Sakata and associates indicated that in their NTG subjects with average IOP, about 12 mm Hg without systemic or topical treatment, the probable incidence of a DH was 31% in approximately five years. NTG and the frequency of a DH detection has been documented to be significantly associated with focal LC defects. Compared to primary open angle glaucoma (POAG) patients with higher IOP, NTG patients are inclined to have more VF and RNFL localized defects.11,20,21 Since focal LC defects are considered to correspond with neuro-retinal rim loss in glaucoma,22,23 to a larger extent factors independent from IOP play a crucial role in the occurrence of a DH in Lower Tension Glaucoma (LTG ) than in patients with higher tension glaucoma.11 Some of the other factors related to the development of a DH include, reactive gliosis, blood perfusion pressure, elevated endothelin I, immunological related damage, blood -brain barrier disruption and any other factors that may damage the integrity of blood vessels and optic nerve laminar structures.7,10,11,22 A proposed membrane -glymphatic theory of primary glaucoma may also influence the formation of a DH.13 The glymphatic system contributes to the regulation of interstitial fluid transport, waste elimination and possibly brain immunity.14 These factors have been identified to cause focal changes to the LC mainly in the more susceptible area inferior temporal and superior temporal that may lead to development of DH.24
Although a DH has been associated with, and are spatially correlated to LC defects, a lack of association between the size of LC defects and a DH suggests an indirect casual relation.9–11 Similarly, Suh and associates reported reduced vessel density in glaucomatous eyes does correlate with the LC defect’s location. They also indicated that loss of laminar support by LC defects may directly or indirectly influence retinal micro-vasculature. Lack of vascular supply conversely may also cause LC defects. They also suggested that an independent axonal loss factor causing reduction of vessel density could not be ruled out.2 Park et al found that the average IOP was not associated with LC defects. However, they indicated that this result could have been due to a higher proportion of NTG subjects in their LC cohort. They further mentioned that although insignificant, the IOP was higher in the eyes of NTG subjects with LC defects compared to those without them and suggested it should be considered a potential risk factor in NTG.11
Progressive visual filed loss has been documented to develop following a DH that corresponds to its location on the optic nerve.14 Yeo-yang and associates indicated that following resolution of a DH, pigment deposition develops at the same site and this finding may be considered a sign of antecedent hemorrhage occurrence.8 They also noticed that progressive VF loss at the DH site occurred in 81.3% of the eyes, but the RNFL was not reduced significantly. Contrary, other evidence suggests that structural changes may precede the development of VF loss.14,15 Yun Hsia and associates documented in their studied glaucoma subjects, that even though the average RNFL thickness was not significantly reduced within two years of occurrence of a DH in the areas considered to be susceptible (inferior or superior of the disc compared to other locations), the sectoral RNFL was significantly diminished within a year. In the non-DH cohort, the average or sectoral RNFL was not altered in the susceptible or non-susceptible disc sites within a year onset of the DH.14 Hyun-Kyung Cho and Kee observed a greater progression for the rate of change of the Bruch’s membrane opening minimum rim width (BOM)-MRW) compared to the rate of RNFL loss in early glaucoma stage eyes with a DH.7 Since there is a relative greater alteration of structural compared to functional tests in early glaucoma, they suggested that BMO-MRW may be more valuable at detecting glaucomatous damage following development of a DH in early glaucoma.
Yeo-Yang and associates have suggested that lowering IOP in NTG may not prevent worsening of visual function and may not be beneficial at preventing VF progression.8 Similarly, the NTG collaborative study indicated that in their NTG subjects’ eyes with a DH, lowering IOP was not beneficial at preventing VF progression.1,25,26 Bengtsson and associates however indicated that lowering IOP after a DH delayed progression of glaucoma1,27 and Medeiros and associate also indicated that lowering IOP may be beneficial at limiting VF progression.1,16 Other investigators also have indicated that intensification of treatment may be advantageous at ameliorating the rate of RNFL thinning and loss at the disc quadrant of a previous DH occurrence.1 They documented in their subjects with glaucoma or glaucoma suspects that had a previous DH, after treatment was intensified, the rate of mean RNFL thinning was slower in the DH quadrant compared with the non-DH quadrant before treatment intensification. Following a DH occurrence, the global, non-DH and DH quadrants rate of RNFL thinning was reduced after DH more than before DH onset in subjects receiving treatment intensification compared to subjects without intensification treatment. In the non-intensified cohort, the rate of RNFL thinning was faster after the DH onset than prior. Some studies have provided documentation that lowering IOP reduced the incidence or frequency of a DH.28,29 Contrary, other investigations found that lowering IOP did not reduce the frequency of a DH and suggested that occurrence of a DH is not indicative of inadequate IOP control.1,25,26
Since the VF was normal in the patient discussed in this case, early indication of progression would not have been possible. The progressive RNFL thinning corresponding to the previous location of the DH, signaled the potential for eventual glaucomatous VF loss. The observation of a superior temporal slit RNFL defect on the optic nerve photos OD proximal to the location of the DH may indicate a previous DH occurrence. Consequently, like the corresponding OCT RNFL thinning progression, this observation may be another indicator of potential VF loss. Although the patient’s maximum IOP during the previous five years was 13 mm Hg, some evidence suggests that further lowering of IOP may be beneficial at reducing RNFL thinning and possible VF progression,1,16 thus commencing treatment was considered. However, the superior, inferior, and average RNFL measurements (107, 109 and 108 ums respectively) were within the normal range. Based on the rate of progression of -2.76 um per year OD and the potential for glaucoma conversion occurring at 75 ums (108-75um /2.76 um/year), it was estimated that in approximately 12 years the patient may convert to glaucoma.17 Consequently, before rushing to treatment it was sensible to obtain a second opinion from a glaucoma specialist. Following that consultation, the Ophthalmologist agreed to continue observation and verifying further RNFL progressive thinning or VF loss before starting treatment.