INTRODUCTION
Epiphora is a very common complaint among the aging patient population. Severity can be variable, ranging from minimal to severe enough to affect activities of daily living. It is critical that providers identify the correct anterior segment underlying pathological cause of epiphora to allow for appropriate management and improvement of patient’s symptoms and well-being.
Epiphora results from lacrimal outflow dysgenesis, which is caused by pathology affecting the lacrimal outflow system.1,2 Unimpeded lacrimal outflow follows a single pathway, which begins with the closure of the palpebral fissures, temporal to medial, during a blink.3 As this occurs, the canaliculi and lacrimal sac contract via Horner’s muscle, which creates negative pressure in which tears are pulled into the punctum and canaliculus and then into the lacrimal sac.4 When the palpebral fissure opens after a blink, the negative pressure draws the tears back into the puncta. Once in the punctum, the lacrimal outflow pathway continues through the canaliculus, lacrimal sac, nasolacrimal duct, and then drains into the nasal cavity.5 If any pathology is present along the nasolacrimal outflow pathway, regurgitation of tears can occur, resulting in epiphora.6 As each cause requires specialized work-up, and different management, it is essential for primary eyecare providers to be able to systematically manage epiphora.
CASE REPORT
A 74-year-old white male presented with a complaint of unilateral epiphora of the right eye which began approximately four to six weeks prior to exam. He stated that it was constant, and greatest when outdoors. He had no additional ocular complaints and denied any history of ocular trauma. Entering visual acuities with correction were 20/20-1 OD, and 20/20-1 OS. Pupils, extraocular movements, and confrontational visual fields were all unremarkable. Intraocular pressure measured by iCare tonometry was 12 mmHg OD and 12 mmHg OS. Pertinent anterior segment exam findings included thickened lid margins OU and trace injection of the bulbar and palpebral conjunctiva OU. Additionally, there were no signs of infection such as the presence of discharge in the eyes. Instillation of sodium fluorescein did not show any staining of either cornea upon instillation of sodium fluorescein there was no indication of keratitis; however, it did show an instant tear break up time OU. The tear meniscus within the lacrimal lake was estimated to be of average size. Upon closer inspection of the lid margins on slit lamp evaluation, it was noted that there were two open puncta in the lower eyelid margin of the right eye, both with good apposition.
The leading cause of the patient’s epiphora was determined to be the presence of supernumerary puncta, in addition to reflex tearing due to dry eye syndrome. Initial treatment with 0.5% carboxymethylcellulose artificial tears QID OU, and warm compresses BID OU was initiated. The patient was educated to return to clinic two weeks later for further assessment of the patency of the nasolacrimal pathway.
ADDITIONAL EXAMINATIONS
Follow Up #1
The first follow up exam was two weeks after initial presentation. Entering acuities were 20/20-2 OD, 20/20-2 OS with all other entrance exam findings being stable. There still were not any signs of infection. Instillation of sodium fluorescein did not show any staining of either cornea upon instillation of sodium fluorescein there was no indication of keratitis, and the tear break up time remained instant OU.
The patient stated that he had some relief of the epiphora of the right eye; however, it was still present and bothersome. Jones I test was performed to assess the patency of the nasolacrimal duct. Trace amount of fluorescein was detected from the right nostril, suggesting patency of the nasolacrimal duct. Jones II testing was not performed as positive patency of the nasolacrimal duct was confirmed.
Schirmer’s testing was performed to assess tear production. Schirmer’s with and without anesthetic was performed, but was inconclusive, as the accumulation of tears was greater without anesthetic than with anesthetic present. This could have been caused by a bolus of reflex tearing, or placing the Schirmer’s testing strip before the proparacaine drop was drained.
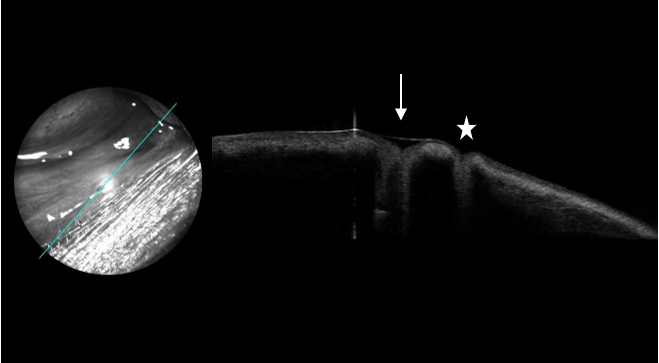
Further assessment included placement of a dilator in each accessory punctum to assess depth. The lateral punctum was deeper as it could be inserted further than with the medial punctum. Imaging of the supernumerary puncta via anterior segment optical coherence tomography (OCT) was also performed (see Figure 1). With both the insertion of the dilator and confirmation with anterior segment OCT, the accessory punctum was determined to be the medial one. The presence of musculature surrounding the punctum was noted on OCT, which determined its functionality.7 These findings aligned with previous case reports of the accessory punctum being medially located, with slit-like appearance, and shallow depth.3 A 0.4mm silicone punctal plug was inserted at this visit into the accessory punctum.
Follow Up #2
The patient reported further improvement of epiphora since combining the use of artificial tears QID in both eyes, and the placement of a punctal plug in the accessory punctum. Entering acuity was 20/20-2 OD and 20/20-2 OS. All other entrance testing were stable. Anterior segment findings were unchanged. The 0.4mm punctal plug was absent from the medial accessory punctum. Instillation of sodium fluorescein did not show corneal staining OU. TBUT remained instant OU. Replacement of the 0.4mm punctal plug was performed and the patient was instructed to continue using 0.5% carboxymethylcellulose QID in both eyes which was satisfactory to the patient and provided best relief.
DISCUSSION
The first description of supernumerary puncta was in 1854 and was credited to MacKenzie et al.7 Incidence is approximately 1 in 60,000.5 Supernumerary puncta are more commonly present in the lower lid, have a slit-like appearance, and are positioned medially.5,7,8 Up to four supernumerary puncta may be present at a time and have been reported in other case report publications.9 As the majority of publications are case reports, the incidence of supernumerary puncta presenting unilaterally compared to bilaterally is unknown, however, a study conducted over 20 years ago by Satchi et al noted 23 patients out of 9,000 had supernumerary puncta in which all cases were unilateral.1
Supernumerary puncta are a congenital anomaly that occurs during embryologic development.5,6,8 During the fifth and sixth weeks of gestation, the nasolacrimal system begins to develop. It begins with the folding of surface ectoderm, which later creates a cord and fuses.7 The cells continue to proliferate and create the lacrimal sac, canaliculi, and nasolacrimal duct.7 It is thought that when multiple epithelial buds occur, either from an autosomal dominant hereditary pattern, or intrauterine factors, supernumerary puncta and other nasolacrimal anomalies can result.6,7,10 Supernumerary puncta may also have shared or separate canaliculi.5,7,11 A shared canaliculus may be determined by probing of the punctum where the probe may be inserting into one punctum and exit through the other. Dacryocystography or dacryoscintigraphy may also be used to identify a shared canaliculus.7 The majority of reported cases of supernumerary puncta are described to have a separate canaliculus for each punctum. However, there have been a few case studies where it has been found that the puncta have a shared canaliculus, which suggests its rarity.7,12 In a case series by Al Saleh et al, two patients with a confirmed shared canaliculus had greater clearance of sodium fluorescein dye and a faster tear break up time, which they concluded the supernumerary punctum with a shared canaliculus may have led to an increased drainage rate.12
Through careful slit lamp examination with lid eversion, providers can detect supernumerary punctum. Identification of which punctum is the accessory one, and which is the primary requires additional examination. The smaller, shallower, and slit-like puncta is usually identified to be the accessory puncta.3,8 By using a punctal dilator, the vertical canaliculus depth can be measured. This provides valuable support in the identification of the accessory puncta.5 With primary punctum that are functional, the punctal dilator can be further inserted. A second way that each punctum can be identified is with anterior segment OCT imaging. By using anterior segment OCT, assessment of the size of the punctal aperture, as well as the depth of the vertical canaliculus can be obtained non-invasively.13 Additionally with anterior segment OCT imaging, the cross-section allows for the epithelial fibrous tissues, and the muscle of Riolan can be identified, in which its presence determines its functionality.13 Observing the hyper-reflectance of the epithelium of the puncta also can help to differentiate between the accessory and primary punctum. The hyper-reflectance shown by the primary puncta will maintain its thickness through the vertical canaliculus, while the accessory punctum will have a “creeping edge” appearance.14 This is illustrated in Figure 1.
_with_presence_of_te.png)
With the presence of supernumerary puncta, reflux of tears through the accessory punctum can occur causing symptoms of unilateral epiphora.7 The presence of musculature surrounding the punctum can help to determine its functionality. In this case, the patient’s anterior segment OCT showed musculature (see Figure 1). Despite determined functionality with the presence of papillae and surrounding musculature, many patients with supernumerary puncta still experience epiphora due to reflux of tears through the accessory puncta due to its smaller anatomy.1,7 Management is directed at decreasing lacrimal outflow dysgenesis via the use of collagen or silicone punctal plugs, or permanent occlusion by punctal cauterization. This allows tears to follow the nasolacrimal outflow system without regurgitation.2 Providers should also understand that patients with supernumerary puncta may also be at a greater risk of developing nasolacrimal duct pathology, such as nasolacrimal duct stenosis and obstruction, in addition to canaliculitis.1,12,15 With knowledge of supernumerary puncta of being a cause of epiphora, clinicians can extend their differential diagnoses to be able to successfully manage the patients symptoms.
CONCLUSION
Epiphora is a frequent chief complaint amongst patients, especially in the elderly population. Through a careful examination and assessment, the root cause of epiphora can be determined, and the appropriate management can be pursued. Although not exceptionally rare, supernumerary puncta may be present and cause epiphora through lacrimal outflow dysgenesis. Supernumerary puncta can be identified easily through slit lamp examination. With probing of the punctum, and through the non-invasive use of anterior segment OCT, one can identify which punctum is the accessory, as well as determine its functionality. In this case, cessation of epiphora was noted after the identification of supernumerary puncta and managed with the insertion of a punctal plug into the patient’s accessory punctum.