
Introduction
Retinal Vein Occlusions (RVOs) in young adults in the absence of underlying vasculopathic diseases require an extensive work up to rule out underlying etiologies such as abnormal clotting factors, medication side effects, or lifestyle risks. Commonly, lifestyle risk factors include cigarette smoking, alcohol consumption, and recreational drug use. Patients often do not recognize vaping or use of electronic cigarettes as a social danger, so unless specifically asked, use of such products often goes unreported. This case demonstrates a strong correlation between retinal vein occlusion and vaping in a young adult with a negative systemic work up.
Case presentation
A 39-year-old Caucasian male presented to the optometry clinic for a comprehensive eye exam.
The patient had complaints of mild itching but was not using any drops and had no distance or near concerns. The patient had no past ocular history and medical history consisted of controlled sleep apnea and asthma for which he utilized a CPAP machine nightly and an inhaler as needed. Social history was positive for alcohol use rarely.
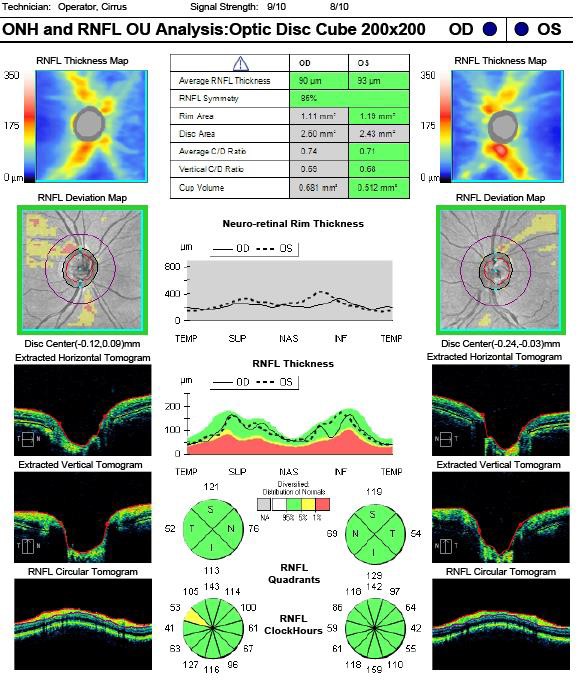
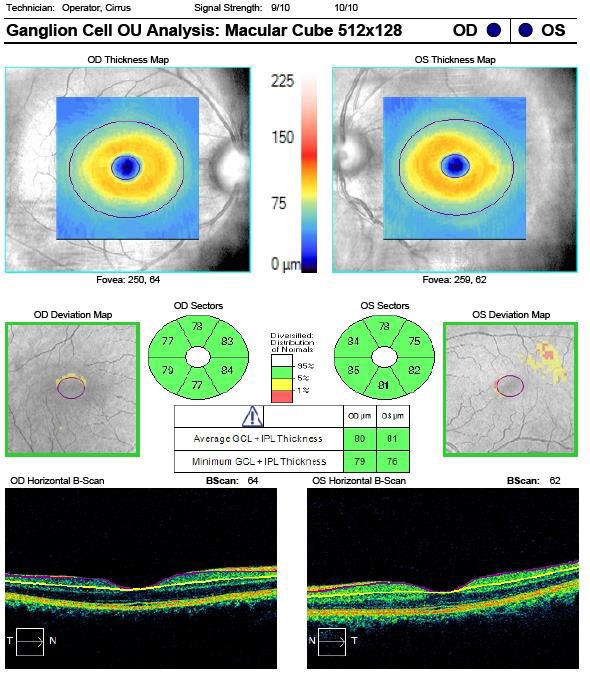
The patient was 20/20 uncorrected OD, OS, OU. Intraocular pressures, extra ocular motilities, confrontation fields, and pupillary testing were all normal. Slit lamp examination revealed 1+ papillae of the palpebral conjunctiva OU and was otherwise normal. Dilated fundus examination revealed subtle dot inter-retinal hemorrhaging which was confluent through the inferior arcade of the left eye. The affected area encompassed nearly one quarter of the total retina, marking most of the posterior pole inferior to the optic nerve. The right eye was normal. Lens and vitreous findings were also normal OU. The patient was diagnosed with a unilateral hemi-retinal vein occlusion without macular edema in the left eye (Image 1). The patient was also diagnosed as a low-risk glaucoma suspect due to slightly larger optic nerve heads. Fortunately, optical coherence tomography showed normal RNFL (image 2), ganglion cell/macular thickness (image 3), and pachymetry were all normal.

The patient disclosed that he vapes regularly and used approximately 1 cartridge per week. He then denied other recreational supplement use, heavy lifting, or other possible lifestyle contributors. The patient was sent to labs and primary care doctor for same day systemic evaluation including a coagulation work-up to determine possible underlying disease such as thrombophilia. The patient was also referred to his pulmonary doctor to determine the stability of his sleep apnea (OSA) and asthma.
Several respiratory tests were conducted, and the patient was determined to be medically stable with appropriate lung function. He receives ongoing treatment with a nightly CPAP machine AirSense 10 Device with Integrated Humidifier.
Systemic evaluation including CBC and physical were normal. FTA, FANA, Cardiolipin antibody panel, Protein S Activity, Antithrombin III, Cryoglobulins, and Factor V Leiden were all within normal limits. Protein C Activity returned at 138.0 with a normal reference range of 70-130. Homocysteine levels returned at 11.8 with a normal reference range of <11.4. Due to the slightly elevated findings, the patient was referred to and seen by our hematology oncology team for a more in-depth analysis.
Hematology/oncology recommended INR and PROTIME labs, lupus anticoagulant and PTT, SPEP with no M spike. All findings were normal, and the hematologist deduced there is no underlying thrombophilia. However, vaping was concluded to be the diagnosis of exclusion, citing increasing clinical evidence suggesting vascular incidents and vaping are linked.
No other analysis was recommended, and the patient was scheduled for follow up in the eye clinic. The patient is currently monitored with gonioscopy and repeat dilations. No neovascularization has occurred to date and the RVO resolved after nine months. The patient discontinued vaping and there has been no recurrence of retinal vein occlusion in either eye since the initial visit.


Discussion
The patient discussed in this paper suffered from sleep apnea (OSA) and asthma, both of which are widely accepted as systemic diseases that can cause vascular disease. However, extensive systemic work up was competed on the patient after RVO diagnosis, and he was determined to be medically stable. Therefore, vaping was determined to be the probable cause of oxidative stress which triggered the patient’s vein occlusion. Vaping is a diagnosis of exclusion which should be considered as a lifestyle risk in patients suffering from ophthalmic vascular disease. As in this case, a thorough systemic work up should be conducted before a diagnosis of exclusion is employed.
Vaping is a somewhat new form of nicotine use that has been advertised as the safer alternative to traditional cigarette use. As more research continues to unfold, it is clear that vaping is not safe. In fact, the ocular risk profiles of both cigarettes and vape use are increasingly similar.
Both cigarette smoke and vaping have been shown to cause oxidative stress leading to endothelial dysfunction and vascular damage despite the main toxins being different.1 Vaping contains mostly formaldehyde and acrolein while the toxic mixture in traditional cigarettes is more complex. A recent study showed no significant difference when comparing the adverse effects of endothelial function between acute vaping and smoking.2
It has been well established that smoking cigarettes is a risk factor for macular degeneration, yet only a few studies have explored this risk association with vaping. Hypoxia in retinal tissue and decreased vascular density were found in a study of electronic cigarettes in otherwise healthy adults.3 In another study, vascular retinal damage was noted when mice were exposed to unflavored nicotine- free vapors with worsening microvascular changes with the use of nicotine vapor.4 Another study highlights various flavored e-liquids induced variable toxicity to RPE cells in the retina.5
Long term use of vaping has been shown to increase platelet aggregation, upregulate adhesion receptors, and impair vascular elasticity, all which have the potential to increase the risk of thrombogenic events.2 Vapes containing nicotine would further increase this risk by significantly increasing heart rate and increasing arterial stiffness.6 Reports show the typical concentration of nicotine in vapes range from 0–36 mg/mL, with some exceeding 56.2 mg/mL7 which is higher than conventional cigarettes.
In a 2019 meta-analysis of global branch and central retinal vein occlusions, the prevalence of branch retinal vein occlusions was found to be 0.23% in people aged 30-39 years compared to 2.64% in those aged 80-89 years.8 Prevalence of any type of retinal vein occlusions was not significantly different between sexes.8 Hypertension and advanced age are the strongest risk factors for a retinal vein occlusion, followed by history of stroke or heart attack. Creatinine and elevated total cholesterol were also identified as risk factors.8
Conclusion
This case suggests patients with preexisting oxidative disorders are at higher risk of vascular complications if vaping is part of the social history. Our patient was a young adult male with well controlled sleep apnea and asthma, who suffered a hemi-retinal vein occlusion. His pulmonary function was within normal range and systemic lab findings were and not suggestive of underlying hypercoagulability. After exclusion of organic causes by multiple specialists, vaping was considered a likely strong contributor to oxidative stress and therefore retinal vein occlusion.
Conflict of Interest and Financial Disclosure
The authors declare that there are no conflicts of interest and no financial ties relevant to the topic at hand.
Acknowledgment
This material is the result of work supported with resources and the use of facilities at the Columbia, South Carolina VA Medical Facility. The authors are employed as optometric physicians for the Columbia, South Carolina VA Medical Facility.
Disclaimer
This content does not represent the views of the U.S. Department of Veterans Affairs or the United States Government.