Introduction
Pseudophakic cystoid macular edema (PCME) is attributed to the disruption of the blood-retinal barrier, leading to fluid buildup within extracellular retinal spaces.1 Clinical observations indicate an approximate incidence rate of 0.6-4.0% in patients with decreased visual acuity following uncomplicated cataract surgery for patients without diabetes or other risk factors.2–4 Historically, fundus fluorescein angiography (FFA) was widely regarded as the standardized method for detecting CME.5 Introducing advanced technology, such as optical coherence tomography (OCT), has provided a rapid and non-invasive means of detecting CME and other retinal conditions with significantly reduced side effects.6
Many ocular and systemic conditions are noted to increase the risk of PCME, one of the major co-morbidities being diabetes.1 Diabetes mellitus presents an elevated susceptibility to cataracts and exacerbates their advancement in affected individuals.7 Considering the inevitability of cataract surgery in such instances, various parameters, such as the length, intensity, type of diabetes, rigidity of the lens, and HbA1C levels, all contribute to the risk assessment.8 A considerable proportion, ranging from 3.2% to 55% of individuals with diabetes, experience PCME after cataract surgery.9,10 This occurrence can be attributed to poor blood-aqueous barrier function within this patient group.11
Case History
A 66-year-old Indian female presented on September 11, 2023, for a dry eye assessment after uncomplicated cataract surgery completed in July and August of 2023. Specifically, the implanted intraocular lens in both eyes was a one-piece monofocal posterior chamber lens; the exact model was unknown. She complained of blurry vision in the distance and near that was persistent from pre-cataract surgery, where her unaided visual acuity before surgery was 20/30 in each eye. She denied pain or discharge. Her medical history was significant for type 2 diabetes (Dx: 2015; 8 mmol/L) and hypertension (130/75 mmHg). Her family history was remarkable for hypertension and diabetes. Her ocular history consisted of evaporative and aqueous deficient dry eye and a history of epiretinal membrane (OD> OS). She had no known drug or environmental allergies. A full eye examination before cataract extraction was completed in December 2022 with no reported ocular complications of diabetes.
Unaided visual acuities status-post surgery were 20/40 in the right and left eye. Subjective refraction did not improve visual acuity (+0.25 / -0.75 x 050 OD and pl / -0.25 x 160 OS). Near visual acuity was 0.4/0.6M OU with +2.50 ADD over the subjective refraction. Schirmer tube measurements were 2 and 3mm in each eye. The ocular surface disease index (OSDI) score was 70.35; before the surgery, it was noted as 25.00 (May 5, 2023).
The current medication list includes ramipril 5mg and Janumet © XR with omega 3, vitamin D, Centrum, and iron. Her dry eye treatments include Hylo ©, Ocunox ©, and Bruder mask ©.
An anterior segment examination revealed meibomian gland dysfunction with inspissated glands, telangiectasia, and an instant tear break-up time. Lids and lashes were clear. Conjunctiva revealed ocular melanosis and conjunctivochalasis OU. Angles were 1.0 (Van Herrick) nasal and temporal. Grade 1+ scattered inferior superficial punctate keratitis (SPK) OD and trace diffuse SPK OS with temporally-located corneal incision scar OU. All other structures were unremarkable without neovascularization of the iris. Intraocular pressures were 10mmHg OD, and 9 mmHg OS. Dilated fundus examination revealed an epiretinal membrane (OD> OS) with no diabetic macular edema. Examination of each intraocular lens revealed well-centred one-piece lens implants with no posterior capsular opacification noted OU. Optic nerves were unremarkable with no neovascularization of the disc or elsewhere. The cup-to-disc ratio was 0.25 H/V OU.
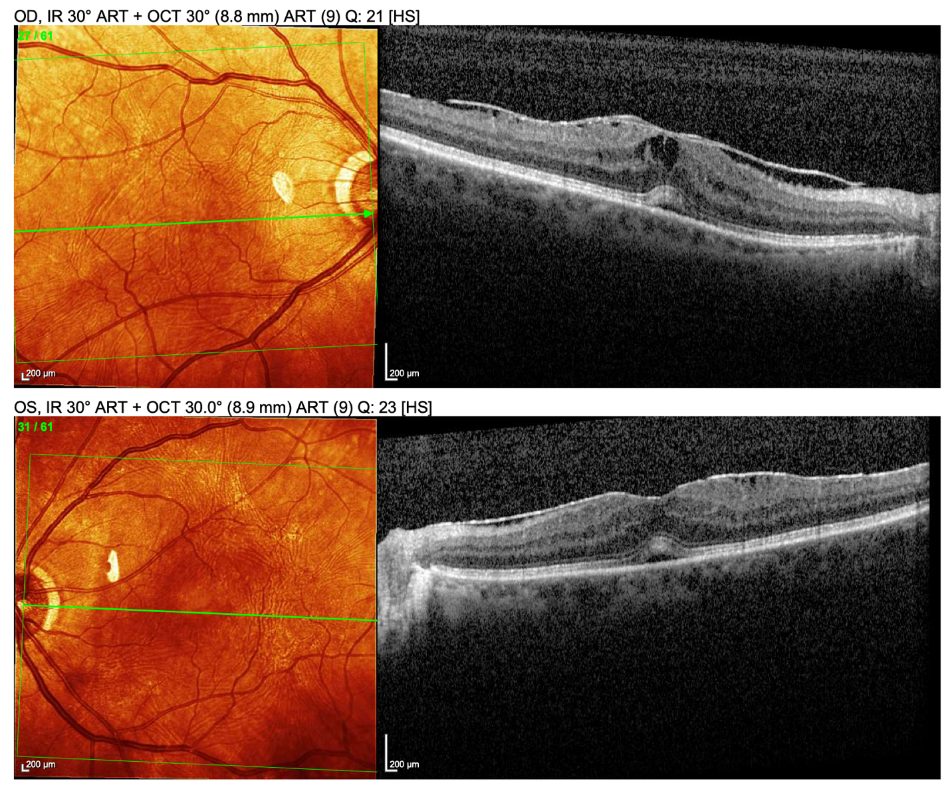
Posterior segment OCT using the Heidelberg Spectralis revealed a mild CME (OD> OS) with sub-retinal fluid (OD = OS) and epiretinal membrane (OD> OS) (which may have caused VA decrease) (Figure I).

The following differential diagnoses were considered:
-
Diabetic macular edema
- Like other etiologies of CME, DME is caused by a disruption in the blood retinal barrier where it results in leakage from microaneurysms and capillaries. Patients affected by DME often carry a history of long-standing diabetes, characterized by persistent elevated or large fluctuations in blood sugar levels. With changes in hyperglycemia, it triggers activation of biochemical pathways and lead to alterations in blood vessels and heightened levels of oxidative stress and inflammation.11–14 This patient had controlled sugar levels with no mention of previous diabetic retinopathy noted. Therefore, DME was deemed an unlikely diagnosis.
-
Pseudophakic cystoid macular edema
- Pseudophakic CME arises from a sudden and localized inflammatory response where it can result in subretinal fluid (SRF) accumulation due to sudden dysfunction of the retinal pigment epithelium, thereby causing a breakdown of the blood-retinal barrier.15 With the proximity of her cataract surgery, appearance of SRF, and bilaterality, PCME was the final diagnosis.
Treatment/Referral
A comprehensive communication was conducted with the patient, elucidating that the probable etiology of her decline in visual acuity stemmed from fluid accumulation within her retinal tissue, a phenomenon not uncommonly seen in diabetic patients who underwent cataract surgery. The patient was referred back to the cataract surgeon for treatment with corticosteroids and NSAID. She was then treated with dexamethasone 0.1% and diclofenac sodium 0.1% QID OU.
Discussion
Cataract surgery is an exceedingly standard procedure fraught with intrinsic postoperative complications. Foremost among these potential complications is pseudophakic cystoid macular edema (PCME), colloquially known as Irvine-Gass syndrome, an adverse event with a proclivity for inducing postoperative vision loss. The exact etiology of PCME post-surgery remains uncertain. However, speculation of the pathophysiology lies within the disturbance of the blood-retinal barrier (BRB), vitreous traction, and prostaglandin release, causing inflammation.15 The peculiarity lies in the timing of PCME incidence, which typically peaks around the fourth to sixth week following an uneventful cataract surgery. The relative risk of PCME increases for previous diagnoses of epiretinal membrane, uveitis, retinal vein occlusion, and diabetes, even without retinopathy.2 The importance of careful postoperative monitoring is emphasized, especially in patients with a background of diabetes and uveitis, as there is a higher correlation of PCME, with estimates citing a four-fold risk compared to patients without diabetes.2
In Canada, Diabetes Mellitus has a prevalence of 8.8% in 2016/2017 with an incidence rate of 603/100,000.16 It has been noted that 30% of Canadians live with diabetes or are pre-diabetic. Individuals afflicted by diabetes mellitus, characterized by an early predilection for cataracts and heightened vulnerability to macular edema (ME) post-cataract surgery, confront a distinctive and formidable clinical conundrum. ME is a significant contributor to unfavourable outcomes in patients with diabetes, primarily driven by oxidative stress induced by hyperglycemia.12 Consequently, the identification of risk factors predisposing these diabetic patients to ME assumes paramount importance, as it empowers clinicians to facilitate early detection, timely intervention, and the implementation of preventive measures.
Differentiating between DME and PCME after surgery poses a considerable challenge. Although there are no distinctive guides to specifically pinpoint the differentiation, patterns have been noted previously to help with the identification. DME typically manifests as a diffuse fluid accumulation where the inner retinal layer cysts (INL) are seen more readily than outer retinal layer cysts (ONL) parafoveally.12,17–19 Although subretinal fluid (SRF) can be found in both cases, without previous notion of diabetic retinopathy, it weighted strongly towards PCME due to its pathophysiology of rapid inflammation onset (table I).17
The treatment options are in accordance with the theorized mechanisms that underlie the etiology of PCME. Corticosteroids and topical nonsteroidal anti-inflammatory drugs (NSAIDs) are the primary first-line treatment modalities.20 In cases where the initial approach proves ineffective, the consideration of intravitreal corticosteroids and anti-VEGF agents comes to the forefront. For chronic PCME and vitreomacular traction (VMT), it may be advisable to consider pars plana vitrectomy as a treatment option.21
The primary focus of the preventative strategy for PCME is reducing surgical complications, shortening surgical length, and carefully utilizing anti-inflammatory pharmaceutical medications. The assessment of therapeutic efficacy for existing anti-inflammatory medicines is challenging due to the frequent occurrence of moderate, spontaneous remission in many patients of PCME.20
Consequently, the precise impact of preventive anti-inflammatory therapies on long-term visual outcomes remains an enigma despite certain studies suggesting potential benefits.20 Hence, meticulous preoperative evaluations are indispensable for categorizing patients as normal or high-risk candidates for cataract surgery.21 Currently, there is no official approved strategy for preventing PCME; however, in some studies, suggestions have been made that preoperative prophylaxis of NSAIDs may be beneficial in preventing PCME.22–24
Previous reports have shed light on cases where individuals with diabetes, following post-cataract surgery, exhibit the coexistence of DME and PCME.12 Microaneurysms, hard exudates, and microfoci have proven helpful in distinguishing between the two conditions. However, their utility becomes less clear when both diseases coexist. Therefore, particularly in such cases, posterior pole findings should always be evaluated in conjunction with other spectral-domain optical coherence tomography (SD-OCT) findings. SD-OCT images can be leveraged for automated classification and by human readers to differentiate between PCME and DME.12,17
Recent studies underscore the significance of optical coherence tomography (OCT) as an indispensable diagnostic tool in addressing these clinical challenges. OCT emerges as an effective instrument capable of detecting postsurgical CME or exacerbations of diabetic macular edema (DME) in diabetic patients, often as early as four weeks post-cataract surgery.17
Conclusion
Individuals diagnosed with diabetes, particularly those with a prior medical history of weak blood-retinal barrier (ie. DR or DME, uveitis) are at an increased susceptibility to PCME after cataract surgery. Differentiation of PCME and DME through SD-OCT and through clinical observation are imperative for determining the appropriate treatment strategy. Proactive interventions have the potential to yield favourable outcomes for individuals at an elevated risk, such as those diagnosed with uveitis or other retinal disorders. It is imperative to provide comprehensive information regarding the patient’s ocular and medical history to the surgeon to facilitate optimal intervention and minimize the risk of PCME.
OCT offers efficiency, safety, and reduced time requirements for detecting CME in diabetic patients undergoing cataract surgery. It allows precise assessment of ME, enabling accurate risk assessment and tailored interventions that enhance overall PCME management, improving visual outcomes and patient care.
Integrations with new technology like OCT have significantly improved diagnostic accuracy and timely interventions, reducing the risk of permanent vision loss. Incorporating advanced ocular imaging modalities into diagnostic and treatment protocols underscores their critical role in clinical practice, enhancing patient care and outcomes as ophthalmology adapts to technological advancements. In a dynamically evolving landscape characterized by technological advancements in ocular imaging, the clinical field of optometry grapples with the complex task of seamlessly integrating these sophisticated instruments into routine practice. This integration gains momentum as extensive documentation accumulates, showcasing their diagnostic prowess across a diverse spectrum of ocular pathologies, thus propelling the frontiers of patient care.