INTRODUCTION
Traumatic optic neuropathy [TON] is a vision-threatening condition that is caused by direct or indirect trauma to the orbit or head. It is suspected that the mechanical shearing forces endured from the traumatic event causes diffuse axonal injury, ischemia, and/or apoptosis of neurons.1 The ocular and visual sequelae of TON may present as uniquely as the individual who exhibits them. Despite the various presentations of TON, all cases will have a relative afferent pupillary defect (with the exception of symmetrical, bilateral cases) and eventual development of optic nerve head findings.1–4 The purpose of this case report is to identify common signs/symptoms of TON, review appropriate in-office tests, and discuss theoretical treatment and management options.
CASE REPORT
A 50-year-old Hispanic male presented for a comprehensive eye exam due to his recent diagnosis of type 2 diabetes mellitus and complaints of blurry near vision. The patient’s past medical history was also comprised of hyperlipidemia, obesity, and chronic post-traumatic stress disorder. His medications included atorvastatin, duloxetine, melatonin, metformin, prazosin, and semaglutide. His last hemoglobin a1c was 7.6 % and last blood pressure was 125/67 mmHg. The patient’s last eye exam was approximately 3-4 years ago. His ocular history consisted of dry eye syndrome and bilateral optic nerve atrophy secondary to a gunshot wound. Per patient history, a bullet had entered his right occipital lobe and exited his left occipital lobe 20+ years prior. Unfortunately, no neuroimaging records were available. He denied history of ocular therapeutics or surgery. His family ocular history was significant for glaucoma and diabetic retinopathy in his grandparents.
Entering visual acuities without correction were 20/20 OD and 20/20-1 OS at distance and 20/40-1 at near OU. The patient was correctable to 20/20 in each eye at distance and near. Extraocular muscles were unrestricted and smooth. Pupils were round and reactive to light with a 1+ relative afferent pupillary defect in the left eye. Visual field testing with frequency doubling technology had one infero-nasal miss in the right eye and four infero-nasal misses in the left eye that was repeatable.
Upon slit lamp examination of the anterior segment, the patient had 1+ meibomian gland dysfunction with inferior papillae concretions and trace mucus strands OU. The corneas displayed trace inferior superficial punctate keratitis. Temporal angles were open to grade 4 Van Herick technique with deep and quiet anterior chambers OU. The irides were flat and brown without neovascularization. The crystalline lenses were clear OU. Intraocular pressures with Goldmann applanation tonometry were 13mmHg in each eye. Central corneal thicknesses were 519 microns OD and 518 microns OS by optical pachymetry.
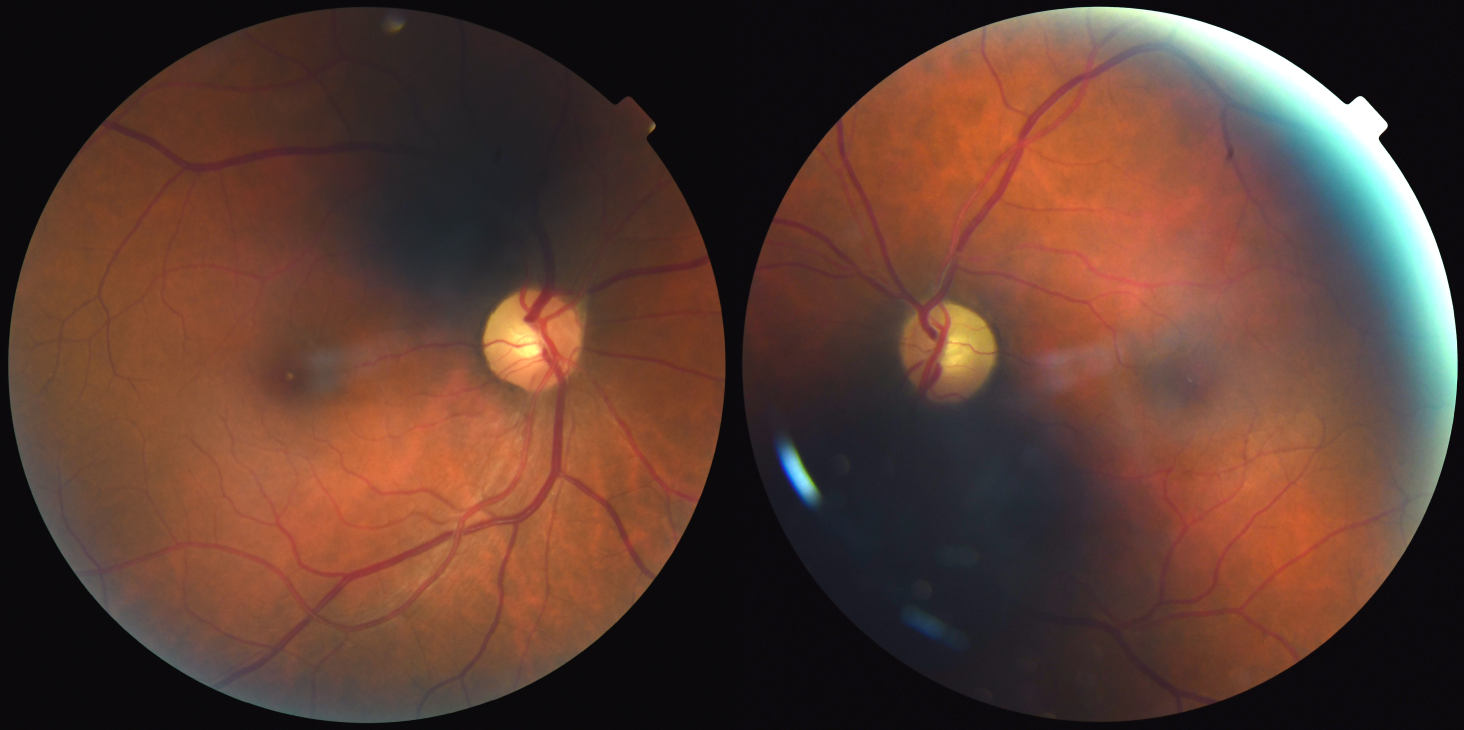
Dilated fundus examination revealed distinct disc margins with superior-temporal rim pallor OD and temporal/superior- temporal/inferior-temporal rim pallor OS without neovascularization of the disc OU (Figure 1). The cup-to-disc ratios were 0.30 round OD and 0.35 round OS in context of average disc size OU. Arteriovenous ratio was 2:3 with normal vascular crossings OU. No retinal hemorrhages, cotton wool spots, intraretinal vascular abnormalities, or neovascularization were appreciated in either eye. Macula and periphery unremarkable OU EMacula and periphery unremarkable OU edema. Bilateral peripheries displayed 360 degrees of white without pressure and were free of holes/breaks/tears.

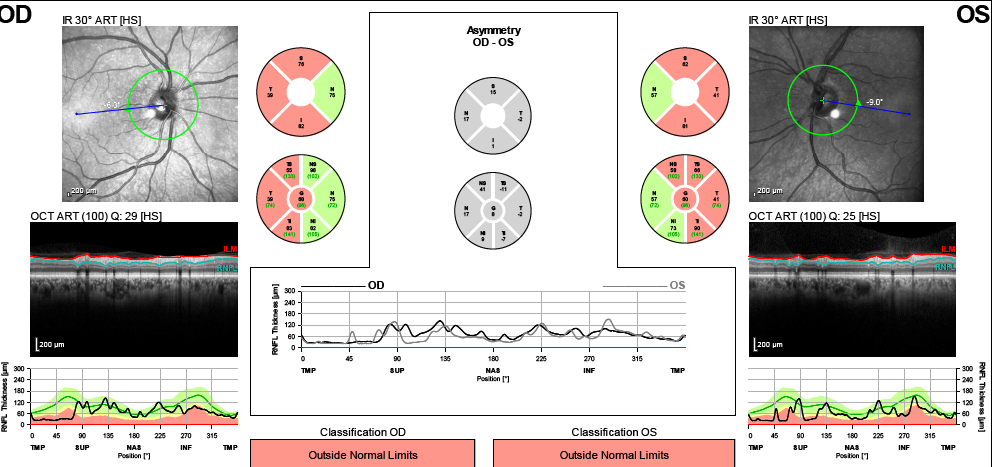
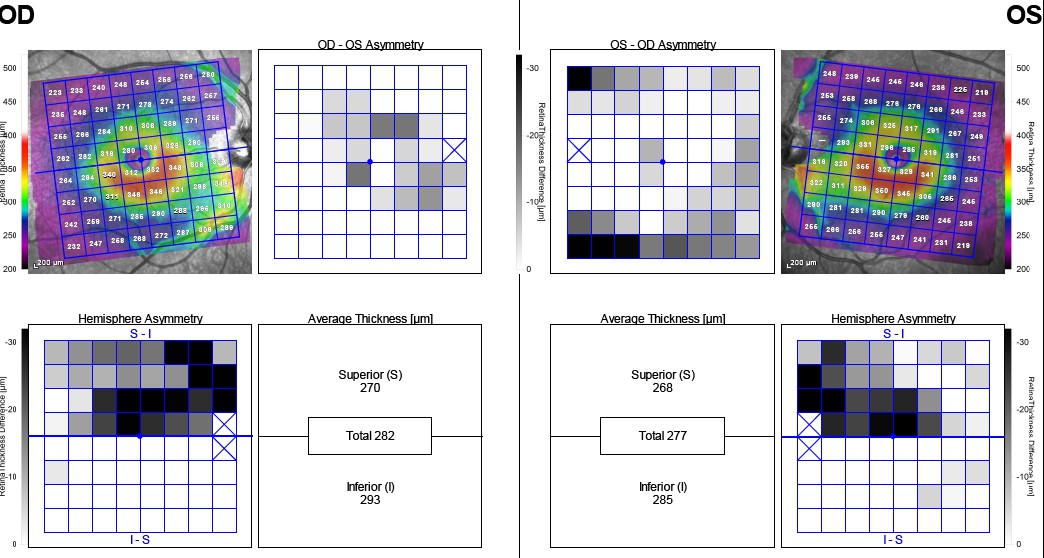
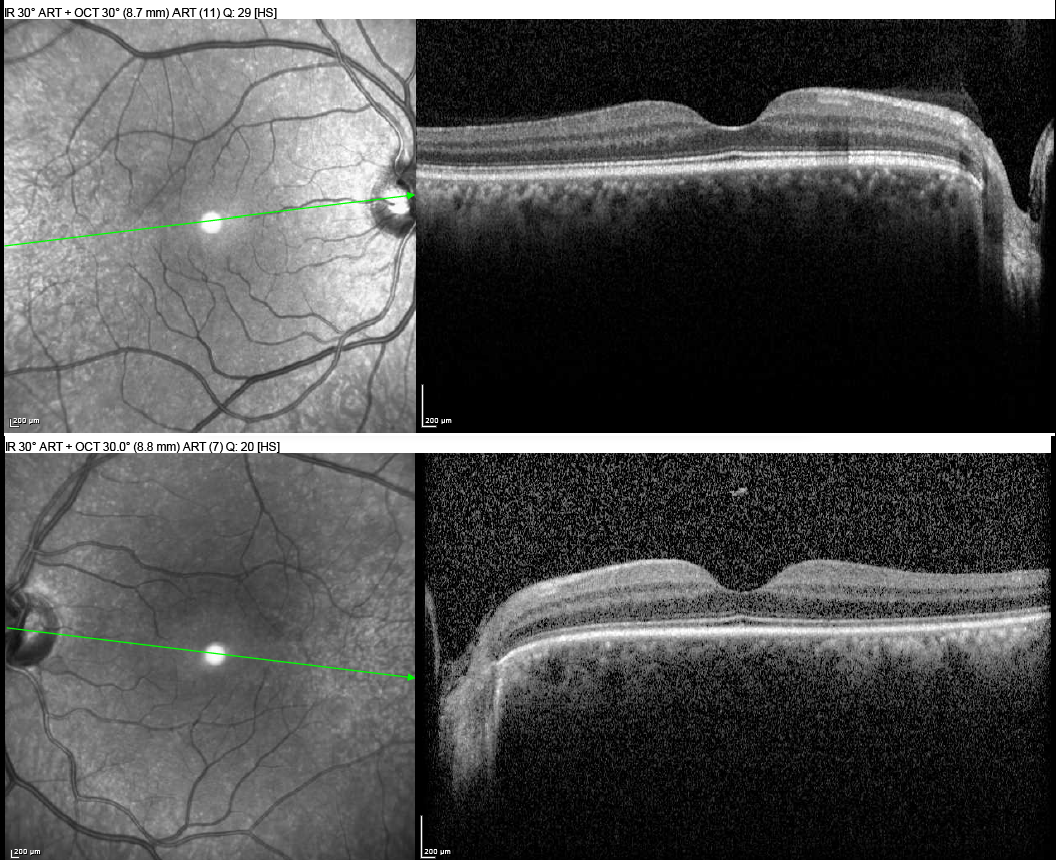
Heidelberg Spectralis optical coherence tomography [OCT] of the optic nerve heads confirmed bitemporal thinning of the retinal nerve fiber layers [RNFL] in the left eye greater than the right eye (Figure 2). Posterior Pole Asymmetry Analysis [PPAA] OCT revealed significant intra- and inter- eye asymmetry with ganglion cell loss more apparent in the left eye than the right eye (Figure 3). OCT scans of the macula were grossly unremarkable in both eyes (Figure 4). All OCT scans were stable to baseline scans from several years ago.



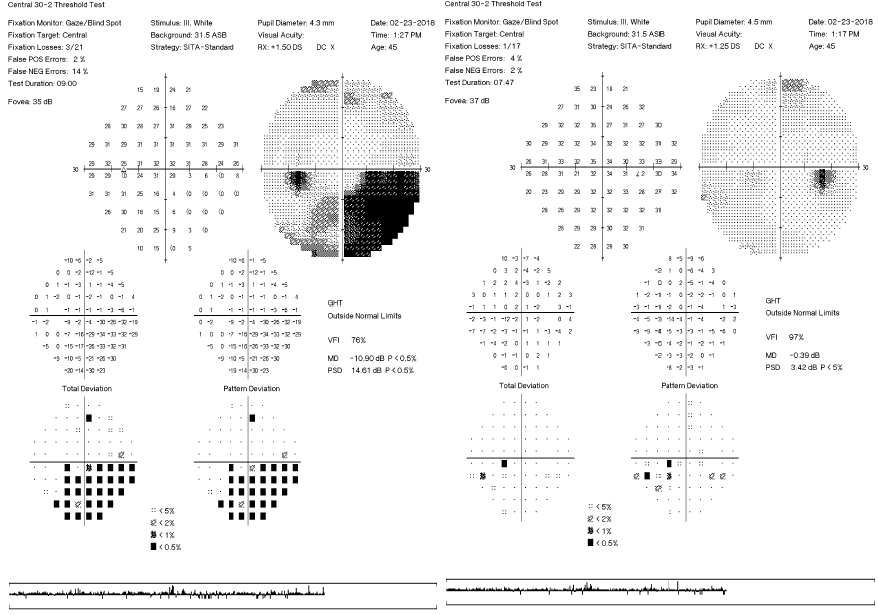
The patient was brought back 2 months after his comprehensive eye exam to update his perimetry testing with the Humphrey Visual Field 30-2 Sita Standard [HVF 30-2 SS] (Figure 5). Both eyes yielded reliable results that correlated with the extent of RNFL thinning apparent on OCT. As seen in Figure 5, there were several depressions in the infero-nasal quadrant of the right eye. The left eye exhibited clusters of absolute defects in the infero-nasal quadrant with several infero-temporal depressions. Overall, the HVF 30-2 SS was stable to baseline perimetry values OU.

The patient’s final assessments were longstanding traumatic optic neuropathy OS> OD secondary to gunshot wound, type 2 diabetes mellitus without retinopathy OU, dry eye syndrome secondary to meibomian gland dysfunction OU, and regular astigmatism OU with presbyopia. The plan for the patient was to monitor TON and T2DM annually with dilated fundus examinations and OCT scans, order artificial tears, and dispense reading glasses.
DISCUSSION
Pathophysiology. Traumatic optic neuropathy [TON] may be classified as primary (direct or indirect) or secondary. Primary TON may be due to direct penetration of or indirect blunt trauma to tissues affecting the optic nerve. Secondary TON includes but is not limited to the following mechanisms: vasospasm, edema or subdural/subarachnoid hemorrhage involving the optic canal, and local compression of vessels or systemic circulatory insufficiency/failure leading to necrosis of the nerve.2,3
Primary indirect TON is more common than direct and secondary TON. The mechanism of injury is like that of traumatic brain injuries. When closed head trauma occurs, the acceleration and deceleration forces may stretch and shear neuronal axons, disrupt the blood-brain barrier, and cause necrotic cell death which may lead to apoptosis.1 Additionally, if blunt trauma is applied to the skull, “deformative stress” may be absorbed by the orbital apex and optic canal.5 These forces may then transmit to the periosteum of the bone where the optic nerve dura fuses and exacerbate swelling and ischemia of the optic nerve via compartment syndrome.5–7
Clinical Diagnosis. Both the afferent and efferent visual pathways may be affected in various ways and magnitudes with TON. To understand the extent of injury and corresponding visual effects, a thorough case history, eye examination, and review of available neuroimaging is necessary.3
History. When inquiring case history, it is important to note when and how the trauma occurred, what materials may have been associated with the injury (e.g. metal or chemical exposure), and any subsequent ocular/visual symptoms.3 This information is particularly useful when ordering ancillary tests such as compound tomography [CT] or magnetic resonance imaging [MRI]. The presence of metallic foreign bodies is contraindicated in MRIs and will cause artifacts in CTs.
Examination. Patients with TON will present with signs/symptoms as unique as the individual themselves. Some TON cases, especially when they are mild, may yield overwhelmingly normal results. TON may be unilateral or bilateral. Visual acuities may range from 20/20 to no light perception. Monocular color vision may or may not be impaired. Static and kinetic perimetry testing may elicit subtle scattered depressions to profound visual field defects.5,8
Despite these unpredictable clinical findings per patient case, the primary tell-tale sign of TON will be the presence of a relative afferent pupillary defect [RAPD] (except in symmetrical, bilateral cases). Many times, a RAPD may be the only abnormal finding in early, acute mild TON cases. If a RAPD is observed, optic nerve pallor and/or atrophy will ensue approximately 6 weeks after the initial traumatic injury.9 Thereafter, one will observe mild to severe optic nerve atrophy with an OCT scan.5
Neuroimaging. CT scans are particularly useful for imaging optic canal and bone fractures, whereas MRIs are helpful in detecting optic nerve and tissue deterioration. Though injury may be apparent in CT or MRI scans, there is no direct correlation between the amount of damage, severity of vision loss, and visual prognosis.10 Due to the inconsistent nature of TON, there is no current consensus on diagnostic neuroimaging.
Treatment. Treatment options for TON include observation, intravenous erythropoietin [EPO], systemic corticosteroids, surgical optic nerve sheath decompression [ONSD], or a combination of the latter; however, there are conflicting outcomes of research. As described in the largest, multi-center study investigating treatment of TON, the International Optic Nerve Trauma Study [IONTS], there is no clear indication of which treatment option is superior. Therefore, it is at the discretion of the provider and patient to determine which course of TON treatment and management is preferred.2,5,10,11
EPO is a cytokine hormone that is secreted from the kidney’s interstitial cells in response to hypoxic or anemic conditions. EPO stimulates hematopoietic stem cells to differentiate into red blood cells and initiates various intracellular cascades with anti- apoptotic, anti-oxidative, and anti- inflammatory effects.12–15 Receptors for EPO can be found throughout endothelial tissue such as the retina’s blood-retinal barrier. Some research shows intravenous EPO reduces “neuronal apoptosis and exert[s] protective effects of mechanical trauma, neuronal inflammation, cerebral and retinal ischemia, oxidative stress, and optic nerve transection” in animal studies.12,16 Conversely, there is insufficient and conflicting evidence in human studies for intravenous EPO improving visual outcomes of TON to a statistically significant level.12
Systemic corticosteroids may be considered for TON treatment due to their ability to minimize inflammation and edema.17 Steroids such as dexamethasone or methylprednisolone are believed to have neuroprotective properties due to their anti- oxidative effects and “inhibition of free-radical-induced lipid peri-oxidation.”12,18 These neuroprotective properties were observed with treatment of spinal cord tissue in the National Acute Spinal Cord Injury Study (NASCIS) and was extrapolated for application to TON; however, the benefits of high-dose corticosteroid treatment in TON are unclear and limited.4,12 A provider must assess and outweigh a patient’s susceptibility to adverse effects of systemic steroids prior to initiation. Adverse effects include, but are not limited to acute psychosis, acute pancreatitis, gastrointestinal bleeding, delayed wound healing, severe sepsis, and severe pneumonia.12
Surgical ONSD may be performed in conjunction with or in lieu of systemic corticosteroids. Surgical ONSD involves the removal of bony fragments that are directly impinging or surrounding the optic nerve.19,20 ONSD can be performed via a transcranial, transantral, intranasal microscopic, or endoscopic approach. The appropriate approach is dictated by the location of impingement. Of note, endoscopic ONSD has a lower risk of morbidity, olfactory preservation, improved scarring cosmesis, and faster recovery time.20,21 “Complete atrophy of the nerve, disruption of the intracranial portion of the [optic nerve], presence of carotid-cavernous fistula, and unstable systemic condition for general anesthesia should be considered as contraindications for any kind of surgical intervention.”4 ONSD application to treat optic neuropathies such as chronic papilledema, pseudotumor cerebri, or TON are highly controversial due to potential complications including cerebrospinal fluid leakage and injury to the ophthalmic artery.20,21
Despite the various treatment options, the results of IONTS and “existing literature provide sufficient evidence to conclude that neither corticosteroids nor optic canal surgery should be considered the standard of care for patients with [TON]. It is therefore clinically reasonable to decide to treat or not treat on an individual patient basis.”22 TON has been found to have a “relatively high rate of spontaneous visual recovery” and no treatment option has proven to be more beneficial than observation alone.5,9–11,16,17,19,23
Prognosis. For direct TON, there is no proven benefit for intervention since vision loss is typically severe and irreversible.9 For indirect TON, there are several predictors of prognosis. The primary predictor is baseline visual acuity – the poorer the acuity, the poorer the outcome. Additionally, visual outcomes will be poor in cases with history of: age greater than 40, loss of consciousness, lack of improvement within 48-hours of injury, blood in the posterior ethmoid cells, intraconal hematoma, and/or a fractured optic canal.4,9
CONCLUSION
Traumatic optic neuropathy is a rare condition that is found in approximately 2.3% -7% of traumatic head injuries.11,23 Examination findings are grossly inconsistent in what is found to be normal or abnormal; however, majority of TON cases will have a RAPD present (except when optic atrophy is bilateral and symmetrical). Due to the variable presentations of TON, treatment and management must be considered on a case-by-case basis. There is currently inconclusive evidence that claims systemic steroids, optic nerve decompression, intravenous erythropoietin, or observation alone, is superior to another. Therefore, the provider and patient must discuss risks, benefits, and their preferred course of action.